

A Japanese lung cancer registry study on demographics and treatment modalities in medically treated patients
- PMID: 32103551
- PMCID: PMC7226207
- DOI: 10.1111/cas.14368
A Japanese lung cancer registry study on demographics and treatment modalities in medically treated patients
Erratum in
-
Correction.Cancer Sci. 2021 Mar;112(3):1332. doi: 10.1111/cas.14831. Cancer Sci. 2021. PMID: 33675173 Free PMC article. No abstract available.
Abstract
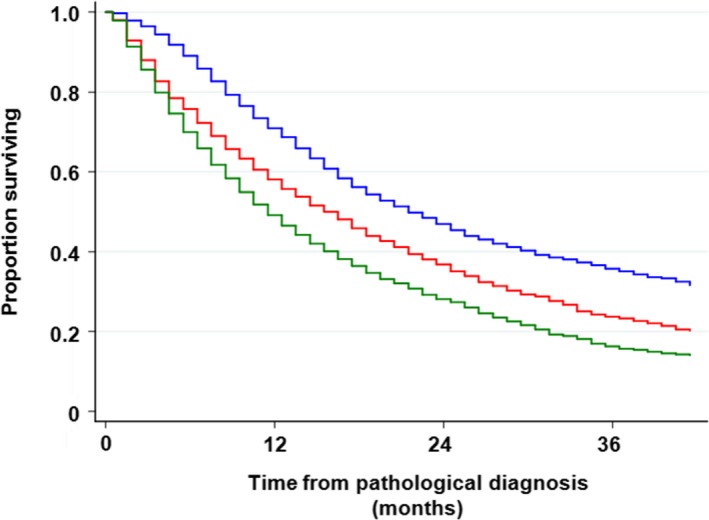
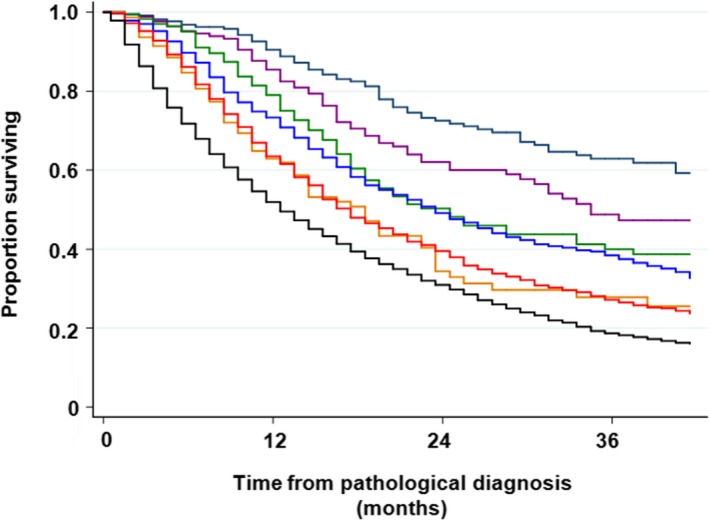
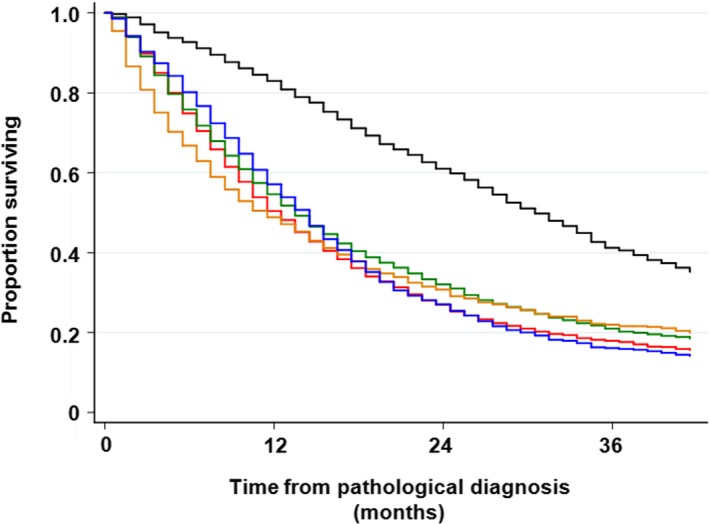
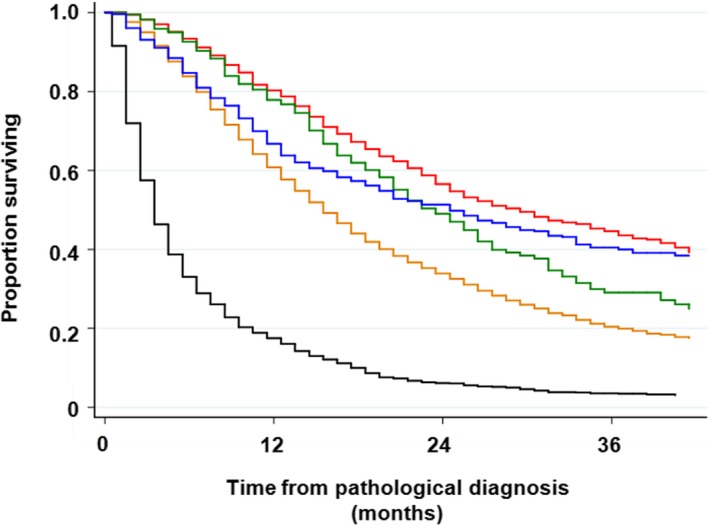
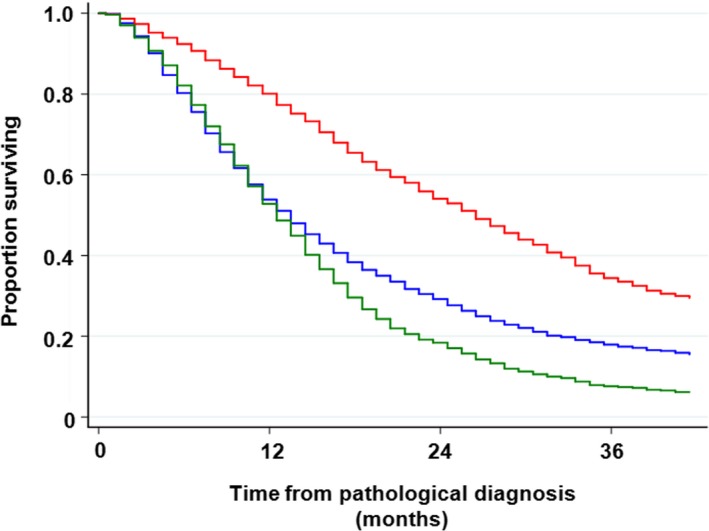
This study provides the benchmark statistics on medically treated patients with non-small cell lung cancer (NSCLC) and small cell lung cancer (SCLC) in Japan. Demographic background, treatment, and prognosis were obtained from patients with lung cancer pathologically diagnosed in 2012, who received nonsurgical treatment. Descriptive statistics and their associations with survival were analyzed. In total, 12 320 patients were registered from 314 institutions in Japan. The median age was 70 years, and 73% of the patients were male. The number (%) of stages I, II, III, and IV diseases were 468 (3.8%), 421 (3.4%), 3260 (26.5%), and 8171 (66.3%), respectively. NSCLC and SCLC accounted for 9872 (80.1%) and 2353 (19.1%) patients, respectively. Thoracic radiotherapy-based therapy, chemotherapy, and palliative care alone were administered to 2572 (20.9%), 7790 (63.2%), and 1952 (15.8%) patients, respectively. Clinical TNM stage was one of the strongest prognostic factors with the 3-year survival rates of 62.9%, 47.3%, 40.0%, 27.8%, 37.5%, 26.5%, and 18.2% for stages IA, IB, IIA, IIB, IIIA, IIIB, and IV, respectively. Among 6158 patients with NSCLC treated with chemotherapy, the 3-year survival rate was 33.4% in patients receiving epidermal growth factor receptor-tyrosine kinase inhibitors (EGFR-TKIs) at some point in their clinical course, whereas it was 17.4% in patients who did not. The 3-year survival rate of SCLC was only 15.9%. In conclusion, approximately two-thirds of the patients were diagnosed as stage IV at the initial diagnosis. Use of EGFR-TKIs significantly improved the survival of patients with NSCLC.
Keywords: TNM stage; epidermal growth factor receptor; non-small cell lung cancer; small cell lung cancer; tyrosine kinase inhibitors.
© 2020 The Authors. Cancer Science published by John Wiley & Sons Australia, Ltd on behalf of Japanese Cancer Association.
Conflict of interest statement
The authors have no conflicts of interest.
Figures
References
-
- Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359‐E386. - PubMed
-
- Goya T, Asamura H, Yoshimura H, et al. Prognosis of 6644 resected non‐small cell lung cancers in Japan: a Japanese lung cancer registry study. Lung Cancer. 2005;50:227‐234. - PubMed
-
- Sawabata N, Asamura H, Goya T, et al. Japanese Lung Cancer Registry Study: first prospective enrollment of a large number of surgical and nonsurgical cases in 2002. J Thorac Oncol. 2010;5:1369‐1375. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
