

Comparing Expert and Non-Expert Assessment of Patients Presenting with Neurological Symptoms to the Emergency Department: A Retrospective Observational Study
- PMID: 32103965
- PMCID: PMC7025652
- DOI: 10.2147/NDT.S236160
Comparing Expert and Non-Expert Assessment of Patients Presenting with Neurological Symptoms to the Emergency Department: A Retrospective Observational Study
Abstract
Objective: Referrals to neurology in emergency departments (ED) are continuously increasing, currently representing 15% of all admissions. Existing triage systems were developed for general medical populations and have not been validated for patients with neurological symptoms.
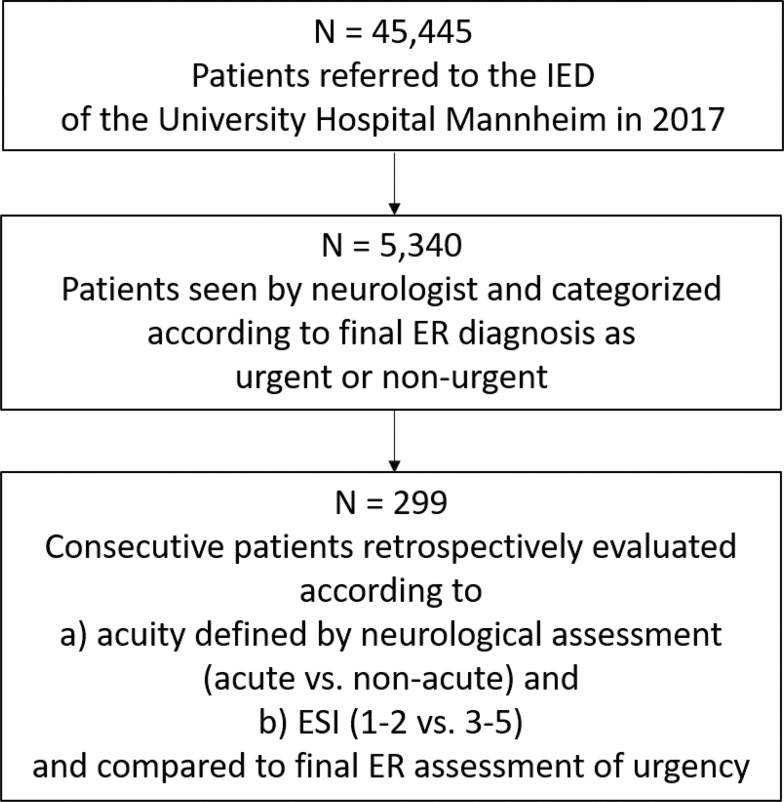
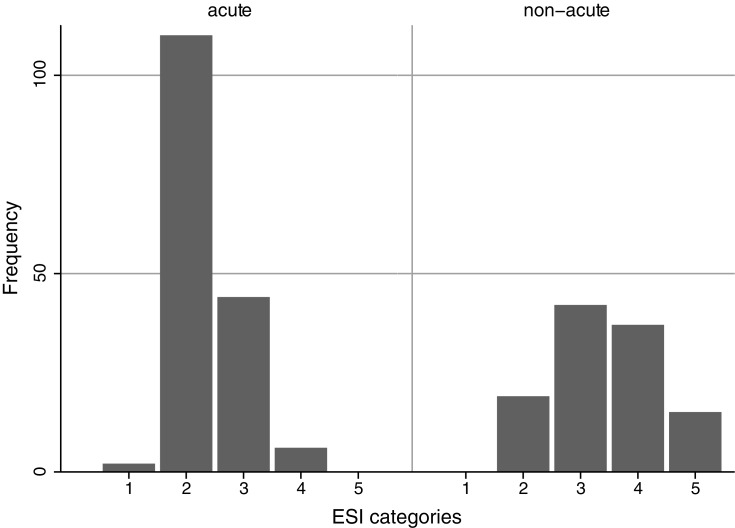
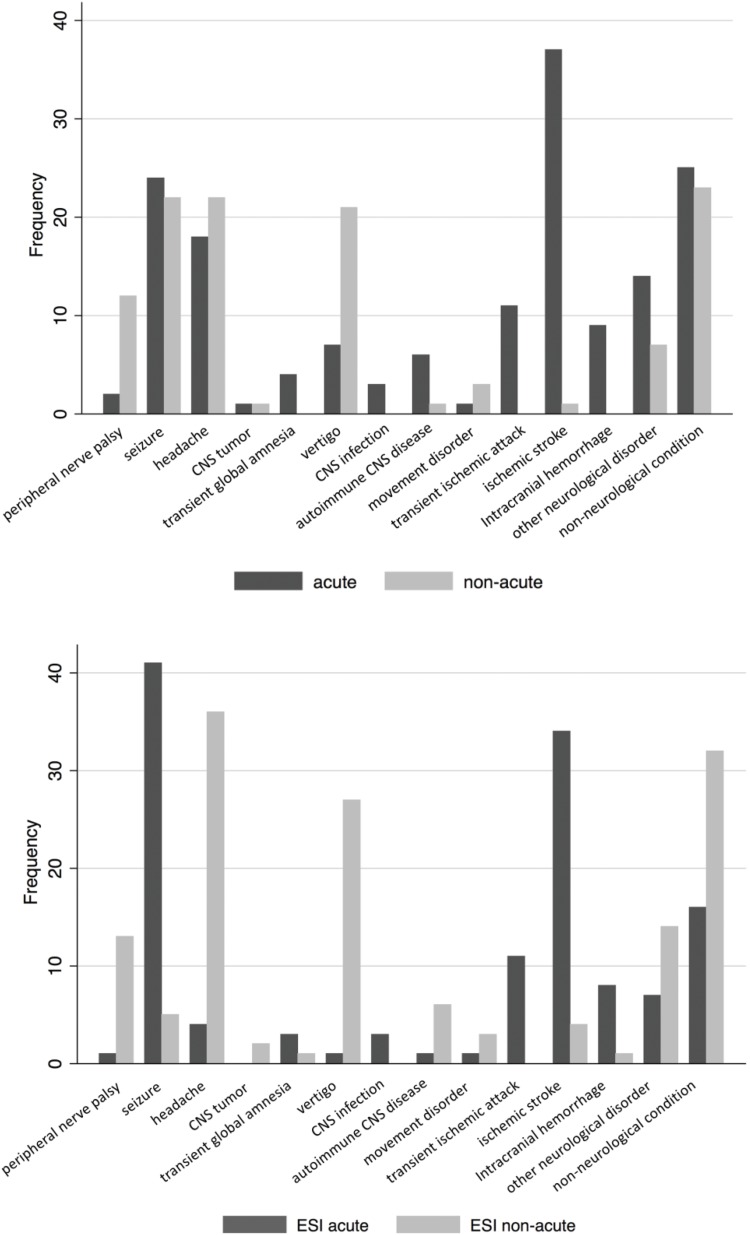
Methods: To characterize neurological emergencies, we first retrospectively analyzed symptoms, service times and resources of the cohort of neurological referrals to a German interdisciplinary ED (IED) during 2017 according to urgency determined by final IED diagnosis. In a second step, we performed a retrospective assignment of consecutive patients presenting in April 2017 according to internal guidelines as either acute (requiring diagnostic/therapeutic procedures within 24 hrs) or non-acute neurological conditions as well as a retrospective classification according to the Emergency Severity Index (ESI). Both assessments were compared with the urgency according to the final ER diagnosis.
Results: In a 12-month period, 36.4% of 5340 patients were rated as having an urgent neurological condition; this correlated with age, door-to-doctor time, imaging resource use and admission (p < 0.001, respectively). In a subset of 275 patients, 59% were retrospectively triaged as acute according to neurological expertise and 48% according to ESI categories 1 and 2. Neurological triage identified urgency with a significantly higher sensitivity (94.8, p < 0.01) but showed a significantly lower specificity (55.1, p < 0.05) when compared to ESI (80.5 and 65.2, respectively).
Conclusion: The ESI may not take specific aspects of neurological emergency (eg, time-sensitivity) sufficiently into account. Refinements of existing systems or supplementation with dedicated neurological triage tools based on neurological expertise and experience may improve the triage of patients with neurological symptoms.
Keywords: emergency; neurology.
© 2020 Hoyer et al.
Conflict of interest statement
Prof. Dr. Simon Nagel reports personal fees from Brainomix, personal fees from Pfizer, grants from Cerenovus, personal fees from Böhringer Ingelheim, outside the submitted work. The authors report no other conflicts of interest in this work.
Figures
References
-
- Schöpke TP. T. Kennzahlen von Notaufnahmen in Deutschland. Notfall Rettungsmed. 2011;14:371–378. doi:10.1007/s10049-011-1435-y - DOI
-
- Wallesch C. Organisation of emergency services in german university and general hospitals - neurological aspects. Aktuelle Neurologie. 2007;34(07):416–421. doi:10.1055/s-2007-971028 - DOI
LinkOut - more resources
Full Text Sources
Miscellaneous
