

Clinical outcomes of blood transfusion to patients with pelvic fracture in the initial 6 h from injury
- PMID: 32104291
- PMCID: PMC7027319
- DOI: 10.3892/etm.2020.8445
Clinical outcomes of blood transfusion to patients with pelvic fracture in the initial 6 h from injury
Abstract
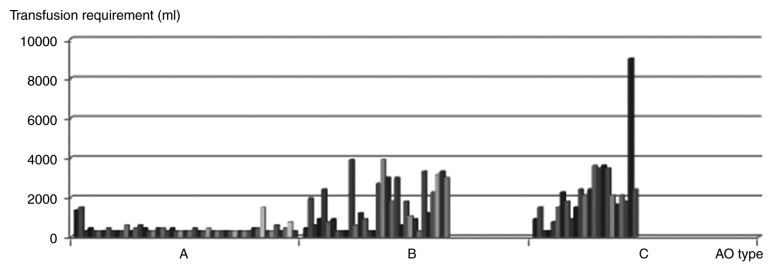
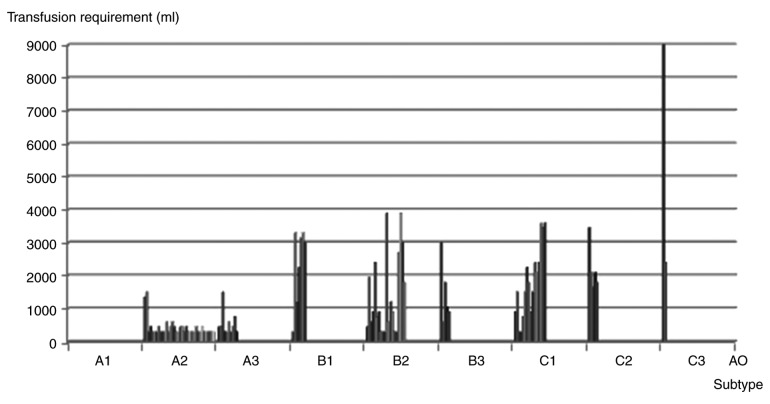
As part of the treatment of pelvic fracture, major hemorrhage poses a challenge for trauma surgeons. The aim of the present study was to evaluate the clinical outcomes of blood transfusion in the initial 6 h after pelvic fracture, and to define the blood transfusion volume required for each pelvic fracture type. A retrospective cohort study was performed on patients with pelvic fracture at a single Level I Trauma Centre over a 3-year period. A total of 1,297 patients were transported to our trauma centre within 2 h of injury and blood transfusion was administered in the initial 6 h after pelvic fracture. Review of the patients' medical records provided the initial pelvic radiographs and data from emergency department care. Clinical outcomes, including frequency of blood transfusion, blood transfusion volume, injury severity scores and mortality, were evaluated. All pelvic fractures were defined as closed fractures and patients were categorized according to the Arbeit fuer Osteosynthese (AO) classification system. Statistical methods were used to identify trends to provide guidance for clinical prediction. Complete data were available for 497 patients with pelvic fracture, 104 (20.9%) of which received blood transfusion. The blood transfusion volume in the initial 6 h ranged from 0 to 10,000 ml, with a mean of 1,213.94±1354.11 ml. The total mortality rate was 1.8%. Among the patients with C-type pelvic fractures, the frequency of blood transfusion was 59.0% and the mean volume was 2,191.30±1,740.93 ml. The mortality rate for C-type pelvic fractures was 11.43%. The B3 subtype of pelvic fractures had the highest transfusion frequency (53.6%), while the C3 subtype had the largest blood transfusion volume (5,700.00±4,666.90 ml). Patients with type A-C pelvic fractures had a progressively larger mean transfusion volume, transfusion frequency and mortality in the initial 6 h after pelvic fracture. The AO classification system was demonstrated to be a useful tool for the identification of pelvic fracture risk in the present study.
Keywords: hemorrhage; pelvic fracture; prediction rule; transfusion.
Copyright: © Yang et al.
Figures
References
-
- Starr AJ, Griffin DR, Reinert CM, Frawley WH, Walker J, Whitlock SN, Borer DS, Rao AV, Jones AL. Pelvic ring disruptions: Prediction of associated injuries, transfusion requirement, pelvic arteriography, complications, and mortality. J Orthop Trauma. 2002;16:553–561. doi: 10.1097/00005131-200209000-00003. - DOI - PubMed
-
- Dalal SA, Burgess AR, Siegel JH, Young JW, Brumback RJ, Poka A, Dunham CM, Gens D, Bathon H. Pelvic fracture in multiple trauma: Classification by mechanism is key to pattern of organ injury, resuscitative requirements, and outcome. J Trauma. 1989;29:981–1002. doi: 10.1097/00005373-198907000-00012. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous