

Utility of Plasma GDF-15 for Diagnosis and Prognosis Assessment of ICU-Acquired Weakness in Mechanically Ventilated Patients: Prospective Observational Study
- PMID: 32104689
- PMCID: PMC7036092
- DOI: 10.1155/2020/3630568
Utility of Plasma GDF-15 for Diagnosis and Prognosis Assessment of ICU-Acquired Weakness in Mechanically Ventilated Patients: Prospective Observational Study
Abstract
Objective: To identify the clinical correlations between plasma growth differentiation factor-15 (GDF-15), skeletal muscle function, and acute muscle wasting in ICU patients with mechanical ventilation. In addition, to investigate its diagnostic value for ICU-acquired weakness (ICU-AW) and its predictive value for 90-day survival in mechanically ventilated patients.
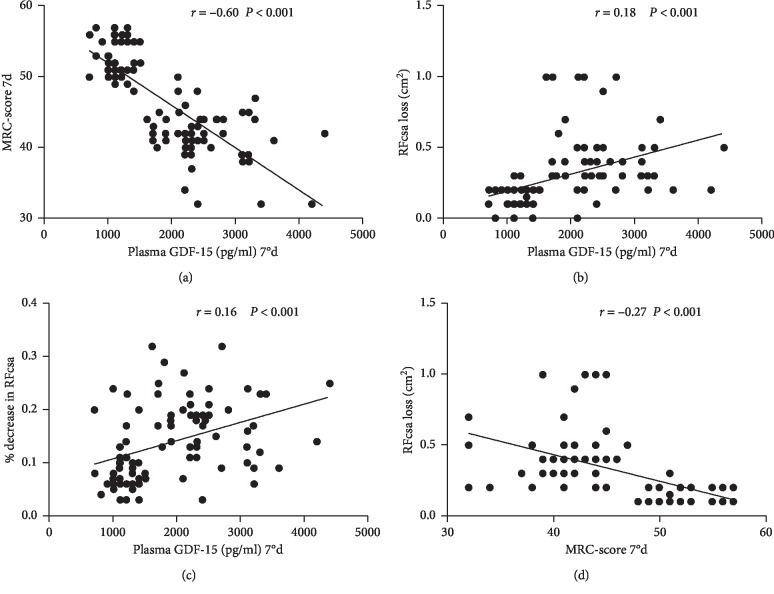
Methods: 95 patients with acute respiratory failure, who required mechanical ventilation therapy, were randomly selected among hospitalized patients from June 2017 to January 2019. The plasma GDF-15 level was detected by ELISA, the rectus femoris cross-sectional area (RFcsa) was measured by ultrasound, and the patient's muscle strength was assessed using the British Medical Research Council (MRC) muscle strength score on day 1, day 4, and day 7. Patients were divided into an ICU-AW group and a non-ICU-AW group according to their MRC-score on the 7th day. The differences in plasma GDF-15 level, MRC-score, and RFcsa between the two groups were compared on the 1st, 4th, and 7th day after being admitted to the ICU. Then, the correlations between plasma GDF-15 level, RFcsa loss, and MRC-score on day 7 were investigated. The receiver operating characteristic curve (ROC) was used to analyze the plasma GDF-15 level, RFcsa loss, and % decrease in RFcsa on the 7th day to the diagnosis of ICU-AW in mechanically ventilated patients. Moreover, the predictive value of GDF-15 on the 90-day survival status of patients was assessed using patient survival curves.
Results: Based on whether the 7th day MRC-score was <48, 50 cases were included in the ICU-AW group and 45 cases in the non-ICU-AW group. The length of mechanical ventilation, ICU length of stay, and hospital length of stay were significantly longer in the ICU-AW group than in the non-ICU-AW group (all P < 0.05), while the other baseline indicators were not statistically significant between the two groups. As the treatment time increased, the plasma GDF-15 level was significantly increased, the ICU-AW group demonstrated a significant decreasing trend in the MRC-score and RFcsa, while no significant changes were found in the non-ICU-AW group. In the ICU-AW group, the plasma GDF-15 level was significantly higher than that in the non-ICU-AW group, while the RFcsa and the MRC-score were significantly lower than those in the non-ICU-AW group (GDF-15 (pg/ml): 2542.44 ± 629.38 vs. 1542.86 ± 502.86; RFcsa (cm2): 2.04 ± 0.64 vs. 2.34 ± 0.61; MRC-score: 41.22 ± 3.42 vs. 51.42 ± 2.72, all P < 0.05), while the other baseline indicators were not statistically significant between the two groups. As the treatment time increased, the plasma GDF-15 level was significantly increased, the ICU-AW group demonstrated a significant decreasing trend in the MRC-score and RFcsa, while no significant changes were found in the non-ICU-AW group. In the ICU-AW group, the plasma GDF-15 level was significantly higher than that in the non-ICU-AW group, while the RFcsa and the MRC-score were significantly lower than those in the non-ICU-AW group (GDF-15 (pg/ml): 2542.44 ± 629.38 vs. 1542.86 ± 502.86; RFcsa (cm2): 2.04 ± 0.64 vs. 2.34 ± 0.61; MRC-score: 41.22 ± 3.42 vs. 51.42 ± 2.72, all r = -0.60), while it was significantly positively correlated with the RFcsa loss (r = -0.60), while it was significantly positively correlated with the RFcsa loss (r = -0.60), while it was significantly positively correlated with the RFcsa loss (r = -0.60), while it was significantly positively correlated with the RFcsa loss (P < 0.05), while the other baseline indicators were not statistically significant between the two groups. As the treatment time increased, the plasma GDF-15 level was significantly increased, the ICU-AW group demonstrated a significant decreasing trend in the MRC-score and RFcsa, while no significant changes were found in the non-ICU-AW group. In the ICU-AW group, the plasma GDF-15 level was significantly higher than that in the non-ICU-AW group, while the RFcsa and the MRC-score were significantly lower than those in the non-ICU-AW group (GDF-15 (pg/ml): 2542.44 ± 629.38 vs. 1542.86 ± 502.86; RFcsa (cm2): 2.04 ± 0.64 vs. 2.34 ± 0.61; MRC-score: 41.22 ± 3.42 vs. 51.42 ± 2.72, all P < 0.05), while the other baseline indicators were not statistically significant between the two groups. As the treatment time increased, the plasma GDF-15 level was significantly increased, the ICU-AW group demonstrated a significant decreasing trend in the MRC-score and RFcsa, while no significant changes were found in the non-ICU-AW group. In the ICU-AW group, the plasma GDF-15 level was significantly higher than that in the non-ICU-AW group, while the RFcsa and the MRC-score were significantly lower than those in the non-ICU-AW group (GDF-15 (pg/ml): 2542.44 ± 629.38 vs. 1542.86 ± 502.86; RFcsa (cm2): 2.04 ± 0.64 vs. 2.34 ± 0.61; MRC-score: 41.22 ± 3.42 vs. 51.42 ± 2.72, all P < 0.05), while the other baseline indicators were not statistically significant between the two groups. As the treatment time increased, the plasma GDF-15 level was significantly increased, the ICU-AW group demonstrated a significant decreasing trend in the MRC-score and RFcsa, while no significant changes were found in the non-ICU-AW group. In the ICU-AW group, the plasma GDF-15 level was significantly higher than that in the non-ICU-AW group, while the RFcsa and the MRC-score were significantly lower than those in the non-ICU-AW group (GDF-15 (pg/ml): 2542.44 ± 629.38 vs. 1542.86 ± 502.86; RFcsa (cm2): 2.04 ± 0.64 vs. 2.34 ± 0.61; MRC-score: 41.22 ± 3.42 vs. 51.42 ± 2.72, all.
Conclusion: The plasma GDF-15 concentration level was significantly associated with skeletal muscle function and muscle wasting on day 7 in ICU patients with mechanical ventilation. Therefore, it can be concluded that the plasma GDF-15 level on the 7th day has a high diagnostic yield for ICU-acquired muscle weakness, and it can predict the 90-day survival status of ICU mechanically ventilated patients.
Copyright © 2020 Yongpeng Xie et al.
Conflict of interest statement
All the authors declare that they have no conflicts of interest.
Figures




References
-
- Patejdl R., Walter U., Rosener S., Sauer M., Reuter D. A., Ehler J. Muscular ultrasound, syndecan-1 and procalcitonin serum levels to assess intensive care unit-acquired weakness. Canadian Journal of Neurological Sciences/Journal Canadien des Sciences Neurologiques. 2019;46(2):234–242. doi: 10.1017/cjn.2018.390. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
