

Pharmacoepidemiology of Ceftazidime-Avibactam Use: A Retrospective Cohort Analysis of 210 US Hospitals
- PMID: 32107536
- PMCID: PMC7884805
- DOI: 10.1093/cid/ciaa061
Pharmacoepidemiology of Ceftazidime-Avibactam Use: A Retrospective Cohort Analysis of 210 US Hospitals
Abstract
Background: Ceftazidime-avibactam has in vitro activity against some carbapenem-resistant gram-negative infections (GNIs), and therefore may be a useful alternative to more toxic antibiotics such as colistin. Understanding ceftazidime-avibactam uptake and usage patterns would inform hospital formularies, stewardship, and antibiotic development.
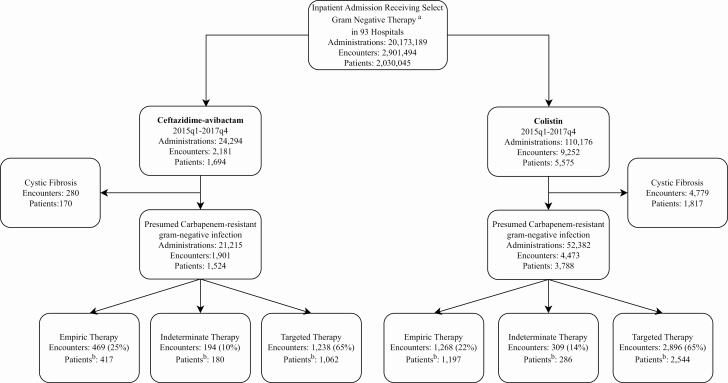
Methods: A retrospective cohort study assessed inpatient encounters in the Vizient database. Ceftazidime-avibactam and colistin administrations were categorized into presumed empiric (3 consecutive days of therapy or less with qualifying exclusions) versus targeted therapy (≥4 consecutive days of therapy) for presumed carbapenem-resistant GNIs. Quarterly percentage change (QPC) using modified Poisson regression and relative change in frequency of targeted ceftazidime-avibactam to colistin encounters was calculated. Factors associated with preferentially receiving targeted ceftazidime-avibactam versus colistin were identified using generalized estimating equations.
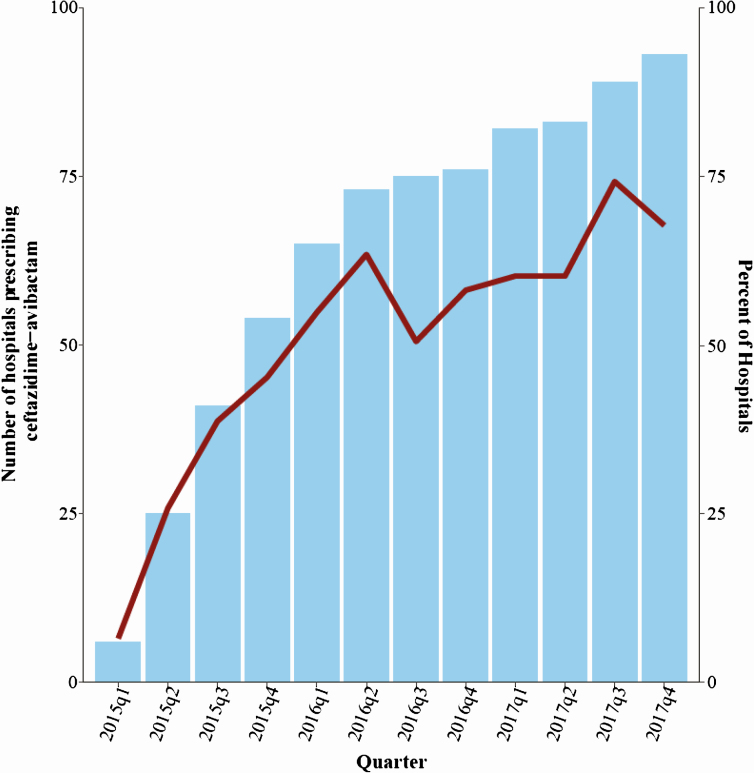
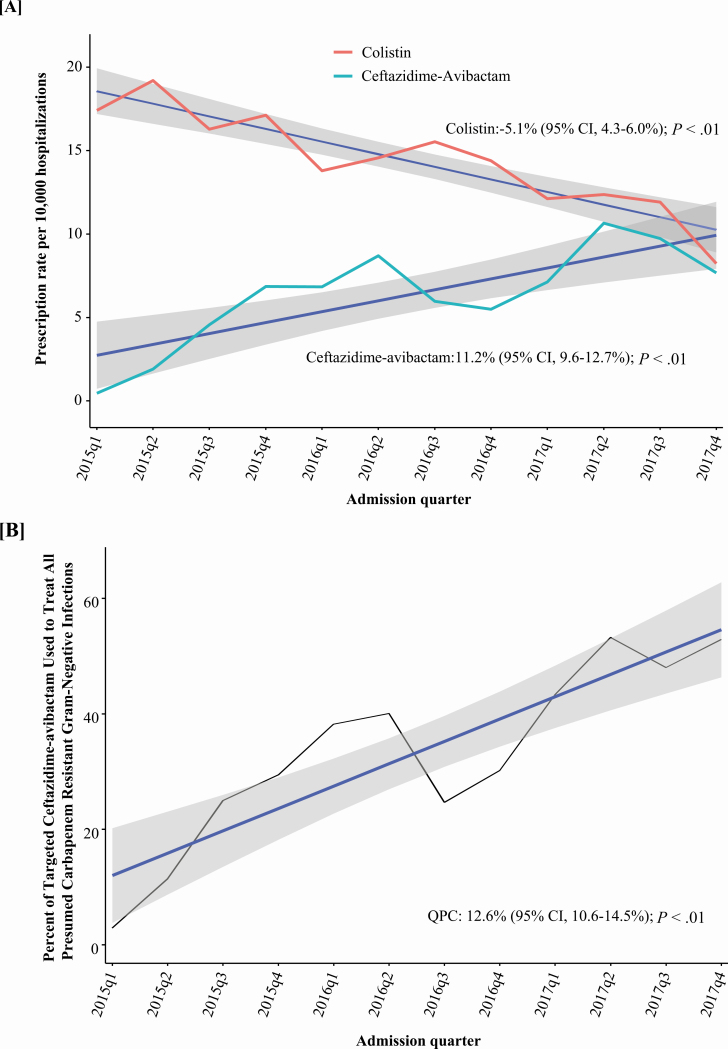
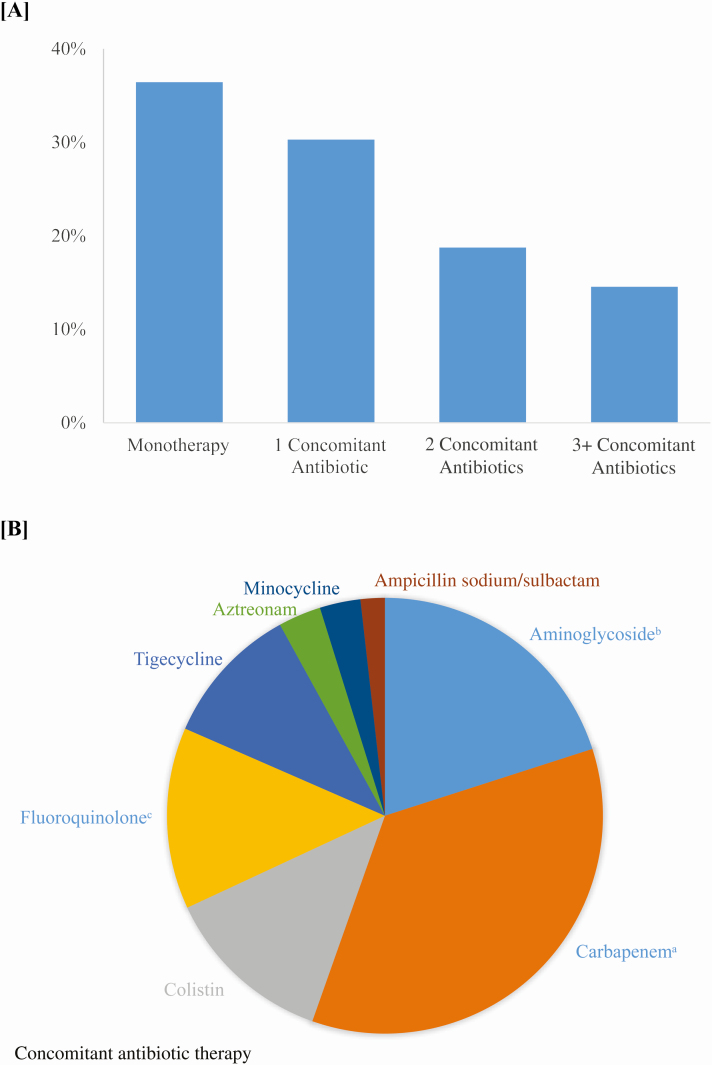
Results: Between 2015 quarter (q) 1 and 2017q4, ceftazidime-avibactam was administered 21 215 times across 1901 encounters. Inpatient prescriptions for ceftazidime-avibactam increased from 0.44/10 000 hospitalizations in 2015q1 to 7.7/10 000 in 2017q4 (QPC, +11%; 95% CI, 10-13%; P < .01), while conversely colistin prescriptions decreased quarterly by 5% (95% CI, 4-6%; P < .01). Ceftazidime-avibactam therapy was categorized as empiric 25% of the time, targeted 65% of the time, and indeterminate 10% of the time. Patients with chronic kidney disease were twice as likely to receive targeted ceftazidime-avibactam versus colistin (RR, 2.02; 95% CI, 1.82-2.25), whereas those on dialysis were less likely to receive ceftazidime-avibactam than colistin (RR, 0.71; 95% CI, .61-.83).
Conclusions: Since approval in 2015, ceftazidime-avibactam use has grown for presumed carbapenem-resistant GNIs, while colistin has correspondingly declined. Renal function drove the choice between ceftazidime-avibactam and colistin as targeted therapy.
Keywords: carbapenem resistance; ceftazidime-avibactam; novel beta-lactamase inhibitors; ram-negative resistance.
Published by Oxford University Press for the Infectious Diseases Society of America 2020.
Figures
Comment in
-
Languid Uptake of Ceftazidime-Avibactam for Carbapenem-Resistant Gram-Negative Infections and Continued Reliance on Polymyxins.Clin Infect Dis. 2021 Feb 16;72(4):622-625. doi: 10.1093/cid/ciaa065. Clin Infect Dis. 2021. PMID: 32107528 No abstract available.
-
Will Ceftazidime-Avibactam Replace Polymyxins in Asia?Clin Infect Dis. 2021 Nov 2;73(9):1743-1744. doi: 10.1093/cid/ciab390. Clin Infect Dis. 2021. PMID: 34009275 No abstract available.
References
-
- Centers for Disease Control. Antibiotic resistance threats in the United States 2019. Available at: https://www.cdc.gov/drugresistance/pdf/threats-report/2019-ar-threats-re...
-
- Theuretzbacher U, Gottwalt S, Beyer P, et al. . Analysis of the clinical antibacterial and antituberculosis pipeline. Lancet Infect Dis 2019; 19:e40–50. - PubMed
-
- Ardal C, Findlay D, Savic M, et al. DRIVE-AB report. Revitalizing the antibiotic pipeline, 2018. Available at: http://drive-ab.eu/wp-content/uploads/2018/01/DRIVE-AB-Final-Report-Jan2...
-
- Falcone M, Paterson D. Spotlight on ceftazidime/avibactam: a new option for MDR gram-negative infections. J Antimicrob Chemother 2016; 71:2713–22. - PubMed
-
- Carr A, Stringer J.. Antibiotic R&D update 20. 2019. Needham Biotechnology. Available at: https://needham.bluematrix.com/sellside/EmailDocViewer?encrypt=06ec2018-...
