

Quantitative analysis of airway obstruction in lymphangioleiomyomatosis
- PMID: 32108050
- PMCID: PMC7330132
- DOI: 10.1183/13993003.01965-2019
Quantitative analysis of airway obstruction in lymphangioleiomyomatosis
Abstract
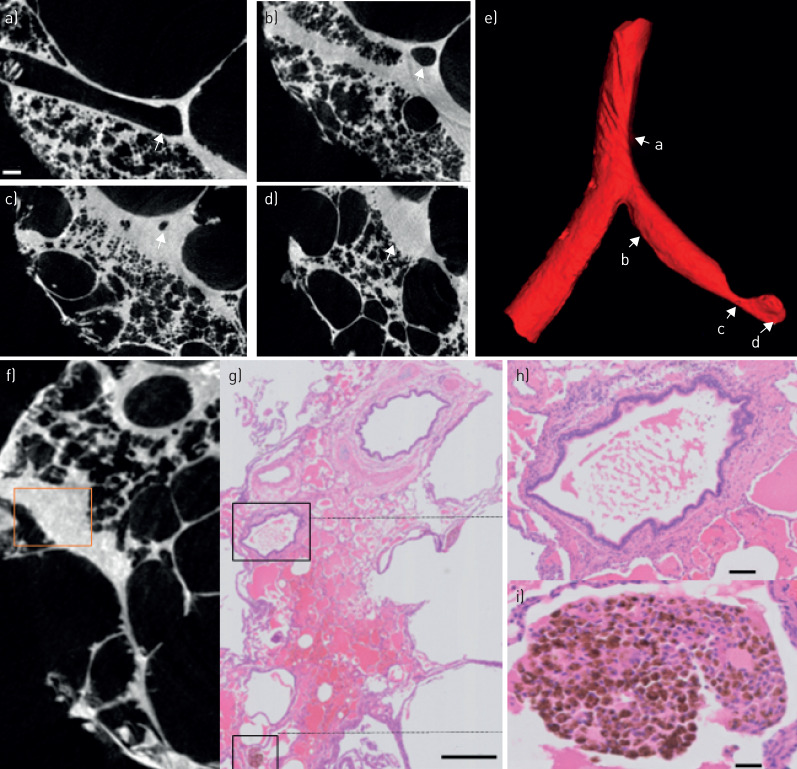
Lymphangioleiomyomatosis (LAM) is a rare, cystic lung disease with progressive pulmonary function loss caused by progressively proliferating LAM cells. The degree of airway obstruction has not been well investigated within the pathogenesis of LAM.Using a combination of ex vivo computed tomography (CT), microCT and histology, the site and nature of airway obstruction in LAM explant lungs was compared with matched control lungs (n=5 each). The total number of airways per generation, total airway counts, terminal bronchioles number and surface density were compared in LAM versus control.Ex vivo CT analysis demonstrated a reduced number of airways from generation 7 on (p<0.0001) in LAM compared with control, whereas whole-lung microCT analysis confirmed the three- to four-fold reduction in the number of airways. Specimen microCT analysis further demonstrated a four-fold decrease in the number of terminal bronchioles (p=0.0079) and a decreased surface density (p=0.0079). Serial microCT and histology images directly showed the loss of functional airways by collapse of airways on the cysts and filling of the airway by exudate.LAM lungs show a three- to four-fold decrease in the number of (small) airways, caused by cystic destruction which is the likely culprit for the progressive loss of pulmonary function.
Copyright ©ERS 2020.
Conflict of interest statement
Conflict of interest: S.E. Verleden has nothing to disclose. Conflict of interest: A. Vanstapel has nothing to disclose. Conflict of interest: L. De Sadeleer has nothing to disclose. Conflict of interest: B. Weynand has nothing to disclose. Conflict of interest: M. Boone has nothing to disclose. Conflict of interest: E. Verbeken has nothing to disclose. Conflict of interest: D. Piloni has nothing to disclose. Conflict of interest: D. Van Raemdonck has nothing to disclose. Conflict of interest: M. Ackermann has nothing to disclose. Conflict of interest: D.D. Jonigk has nothing to disclose. Conflict of interest: J. Verschakelen has nothing to disclose. Conflict of interest: W.A. Wuyts has nothing to disclose.
Figures






Comment in
-
LAM is another small airway disease: lessons from microCT.Eur Respir J. 2020 Jul 2;56(1):2002162. doi: 10.1183/13993003.02162-2020. Print 2020 Jul. Eur Respir J. 2020. PMID: 32616551 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical