

Randomized Phase II Study of First-Line Cladribine With Concurrent or Delayed Rituximab in Patients With Hairy Cell Leukemia
- PMID: 32109194
- PMCID: PMC7213585
- DOI: 10.1200/JCO.19.02250
Randomized Phase II Study of First-Line Cladribine With Concurrent or Delayed Rituximab in Patients With Hairy Cell Leukemia
Abstract
Purpose: Single-agent purine analog, usually cladribine, has been the standard first-line therapy of hairy cell leukemia (HCL) for 30 years. High complete remission (CR) rates often include minimal residual disease (MRD), leading to relapse and repeated treatments. Rituximab can clear MRD, but long-term results are unknown and optimal timing of rituximab undefined.
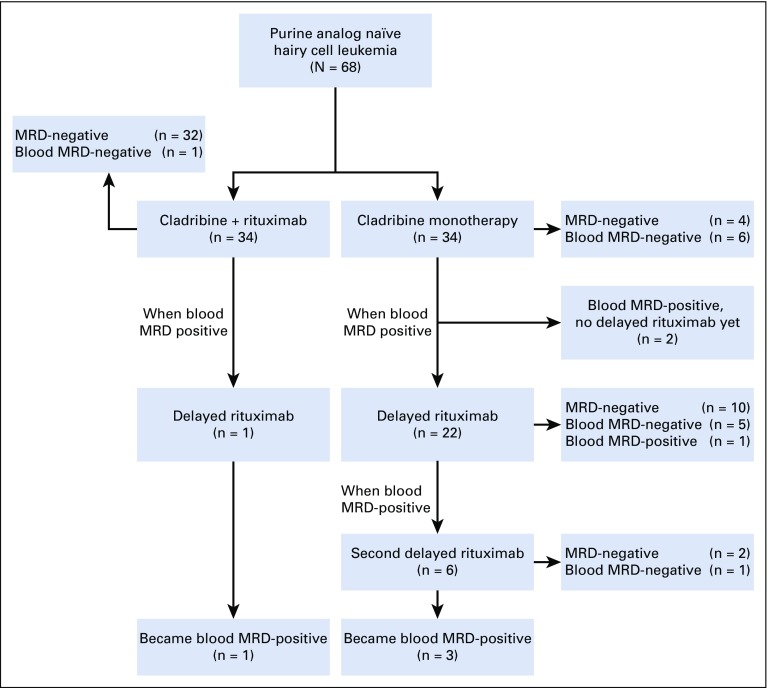
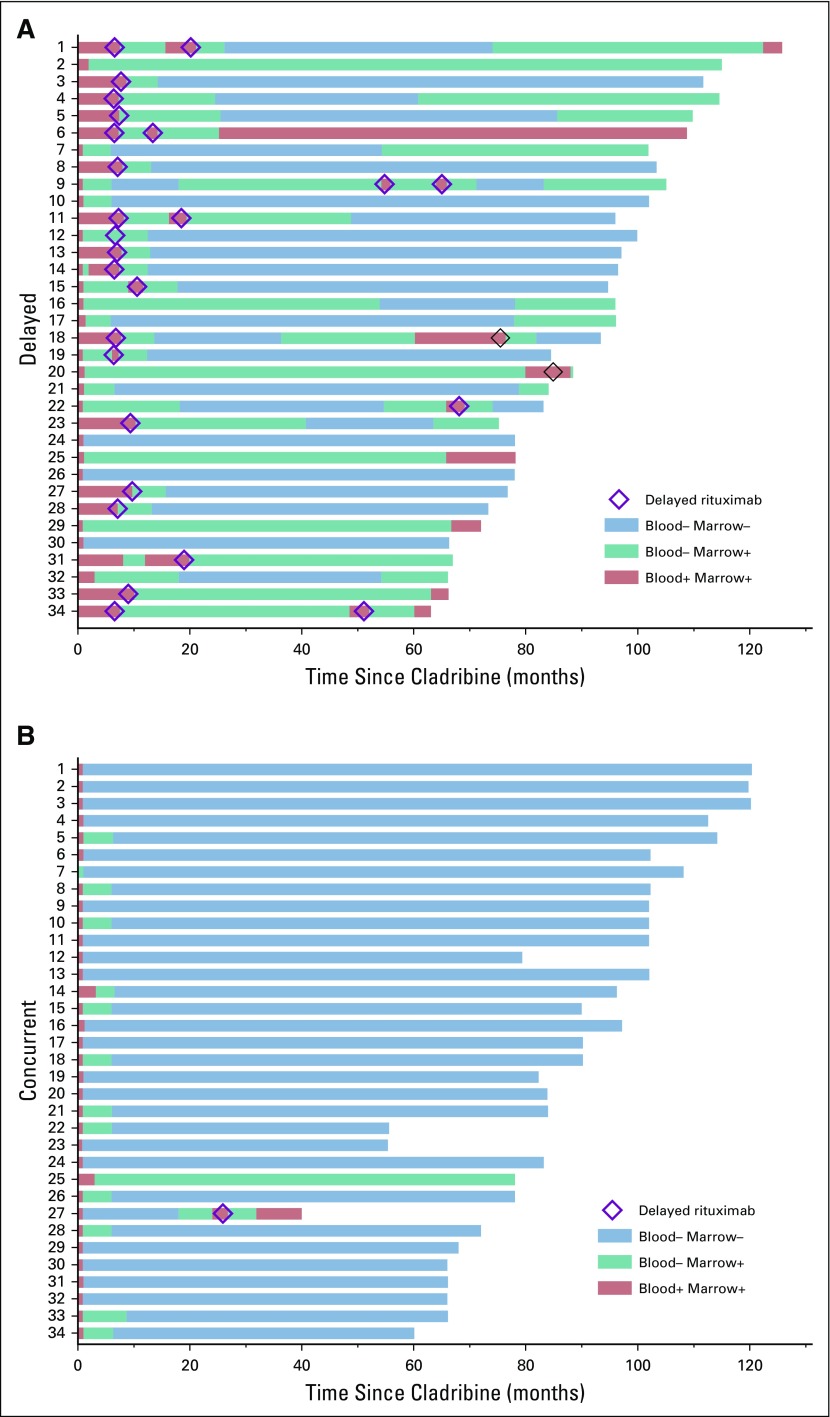
Patients and methods: Patients were randomly assigned to first-line cladribine 0.15 mg/kg intravenously days 1-5 with 8 weekly doses of rituximab 375 mg/m2 begun either day 1 (concurrent, CDAR) or ≥ 6 months later (delayed) after detection of MRD in blood. MRD tests included blood and bone marrow (BM) flow cytometry, and BM immunohistochemistry.
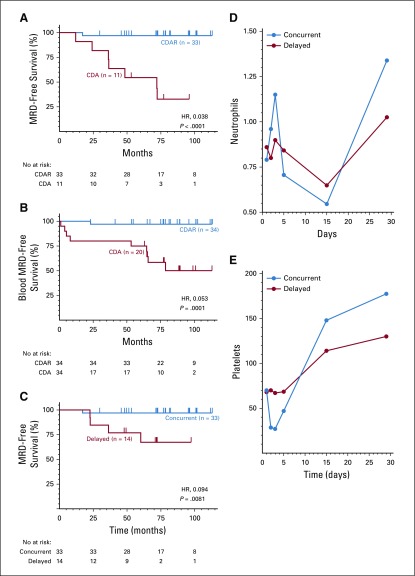
Results: Sixty-eight patients with purine analog-naïve classic HCL were randomly assigned 1:1 to concurrent versus delayed arms. At 6 months after CDAR versus cladribine monotherapy, CR rates were 100% versus 88% (P = .11), MRD-free CR rates 97% versus 24% (P < .0001, primary end point), and blood MRD-free rates 100% versus 50% (P < .0001), respectively. At 96 months median follow-up, 94% versus 12% remained MRD free. Compared with CDAR, delayed rituximab after cladribine achieved lower rate (67% of 21 evaluable patients; P = .0034) and durability (P = .0081, hazard radio favoring CDAR, 0.094) of MRD-free CR. Nevertheless, 12 patients in the delayed arm remained MRD free when restaged 6-104 (median, 78) months after last delayed rituximab treatment. Compared with cladribine monotherapy, CDAR led to brief grade 3/4 thrombocytopenia (59% v 9%; P < .0001) and platelet transfusions without bleeding (35% v 0%; P = .0002), but higher neutrophil (P = .017) and platelet (P = .0015) counts at 4 weeks.
Conclusion: Achieving MRD-free CR of HCL after first-line cladribine is greatly enhanced by concurrent rituximab and less so by delayed rituximab. Longer follow-up will determine if MRD-free survival leads to less need for additional therapy or cure of HCL.
Trial registration: ClinicalTrials.gov NCT00923013.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69:7–34. - PubMed
-
- Teras LR, DeSantis CE, Cerhan JR, et al. 2016 US lymphoid malignancy statistics by World Health Organization subtypes. CA Cancer J Clin. 2016;66:443–459. - PubMed
-
- Else M, Dearden CE, Matutes E, et al. Long-term follow-up of 233 patients with hairy cell leukaemia, treated initially with pentostatin or cladribine, at a median of 16 years from diagnosis. Br J Haematol. 2009;145:733–740. - PubMed
-
- Saven A, Burian C, Koziol JA, et al. Long-term follow-up of patients with hairy cell leukemia after cladribine treatment. Blood. 1998;92:1918–1926. - PubMed
-
- Grever M, Kopecky K, Foucar MK, et al. Randomized comparison of pentostatin versus interferon alfa-2a in previously untreated patients with hairy cell leukemia: An intergroup study. J Clin Oncol. 1995;13:974–982. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
