

Segmental Bioelectrical Impedance Spectroscopy to Monitor Fluid Status in Heart Failure
- PMID: 32109235
- PMCID: PMC7046702
- DOI: 10.1038/s41598-020-60358-y
Segmental Bioelectrical Impedance Spectroscopy to Monitor Fluid Status in Heart Failure
Abstract
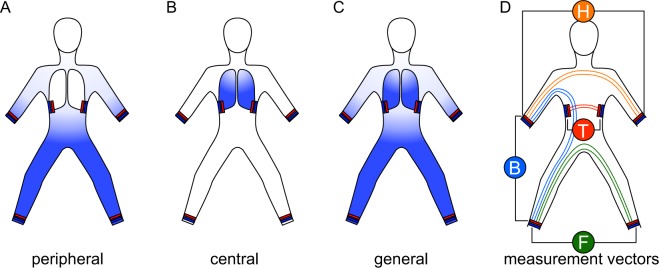
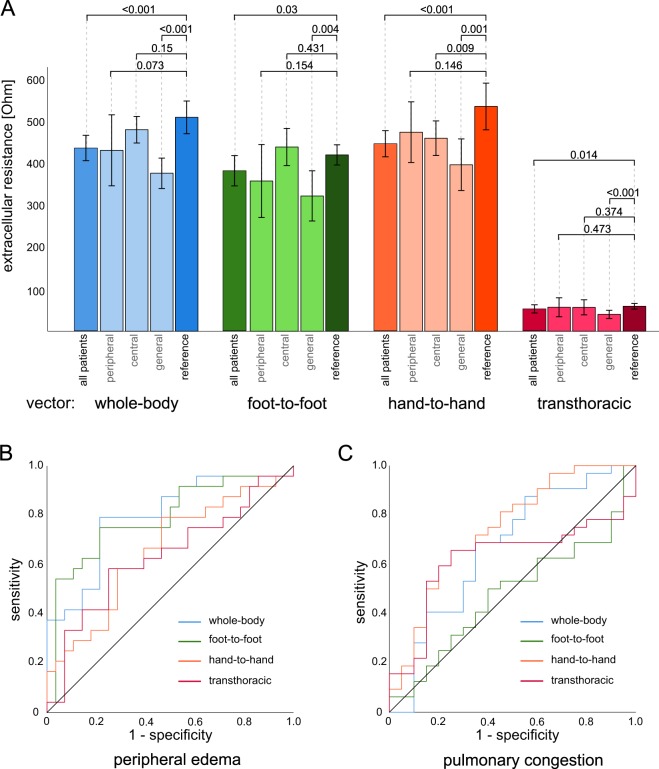
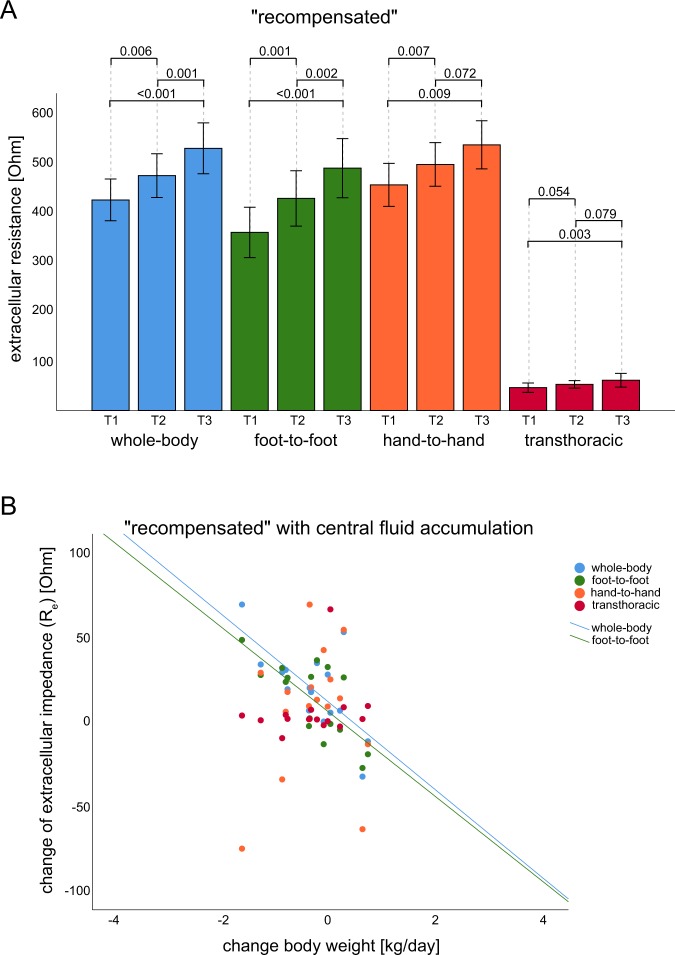
Bioelectrical impedance spectroscopy (BIS) measures body composition, including fluid status. Acute decompensated heart failure (ADHF) is associated with fluid overload in different body compartments. This investigation aimed to evaluate the feasibility of measuring and monitoring fluid accumulation in patients with ADHF using BIS. The extracellular impedance as a surrogate marker for fluid accumulation was measured in 67 participants (25 healthy reference volunteers and 42 patients admitted with ADHF) using BIS in the "transthoracic", "foot-to-foot", "whole-body" and "hand-to-hand" segments. At baseline, BIS showed significantly lower extracellular resistance values for the "whole-body" (P < 0.001), "foot-to-foot" (P = 0.03), "hand-to-hand" (P < 0.001) and "transthoracic" (P = 0.014) segments in patients with ADHF than the reference cohort, revealing a specific pattern for peripheral, central and general fluid accumulation. The "foot-to-foot" (AUC = 0.8, P < 0.001) and "hand-to-hand" (AUC = 0.74, P = 0.04) segments indicated compartments of fluid accumulation with good prediction. During cardiac recompensation, BIS values changed significantly and were in line with routine parameters for monitoring ADHF. Mean bodyweight change per day correlated moderately to good with BIS values in the "whole-body" (r = -0.4), "foot-to-foot" (r = -0.8) and "transthoracic" (r = -0.4) segments. Based on our analysis, we conclude that measuring and monitoring fluid accumulation in ADHF using segmental BIS is feasible and correlates with clinical parameters during recompensation.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Ponikowski P, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016;37:2129–2200. doi: 10.1093/eurheartj/ehw128. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
