

Antibiotic prescribing and outcomes in cancer patients with febrile neutropenia in the emergency department
- PMID: 32109264
- PMCID: PMC7048306
- DOI: 10.1371/journal.pone.0229828
Antibiotic prescribing and outcomes in cancer patients with febrile neutropenia in the emergency department
Abstract
Introduction: The benefit of reducing the time of antibiotic initiation in the emergency department (ED) for neutropenic patients is controversial and the research on the impact of antibiotic adherence to international guidelines in the ED is scarce. We aimed to investigate the effect of antibiotic timing and appropriateness on outcomes in patients with febrile neutropenia (FN) and to assess the performance of the MASCC risk-index to risk-stratify such patients in the ED.
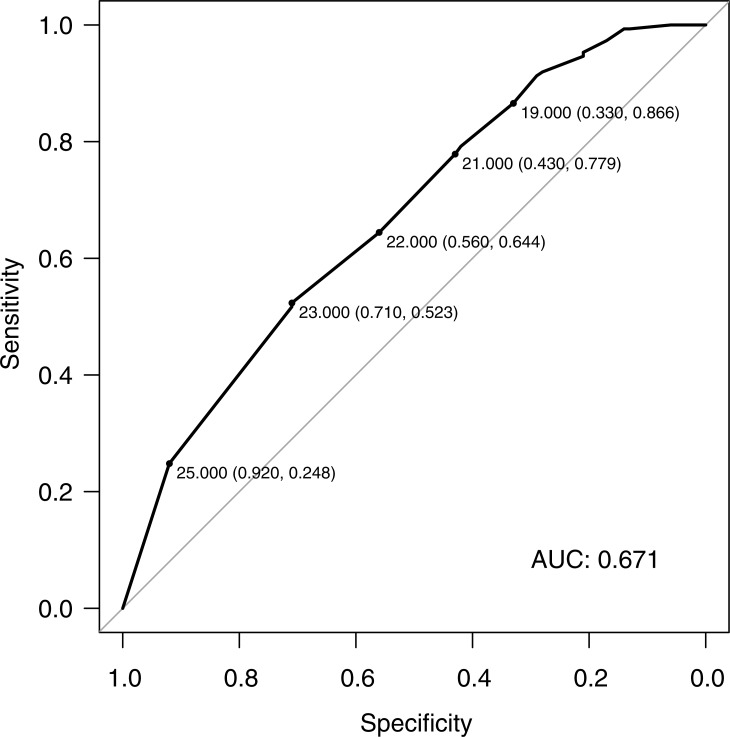
Methods: We prospectively identified patients with FN who presented to our ED and assessed their Multinational Association of Supportive Care in Cancer (MASCC) risk-index. The time to parenteral antibiotic initiation and the appropriateness of the antibiotic regimen according to international guidelines were retrospectively abstracted. The performance of the MASCC risk-index in predicting the absence of complication was assessed with sensitivity, specificity and the area under the receiver operating characteristics curve (AUC). We investigated the effect of the time to antibiotic initiation and the appropriateness of the antibiotic regimen on the outcome (ICU admission or death) by logistic regression analyses.
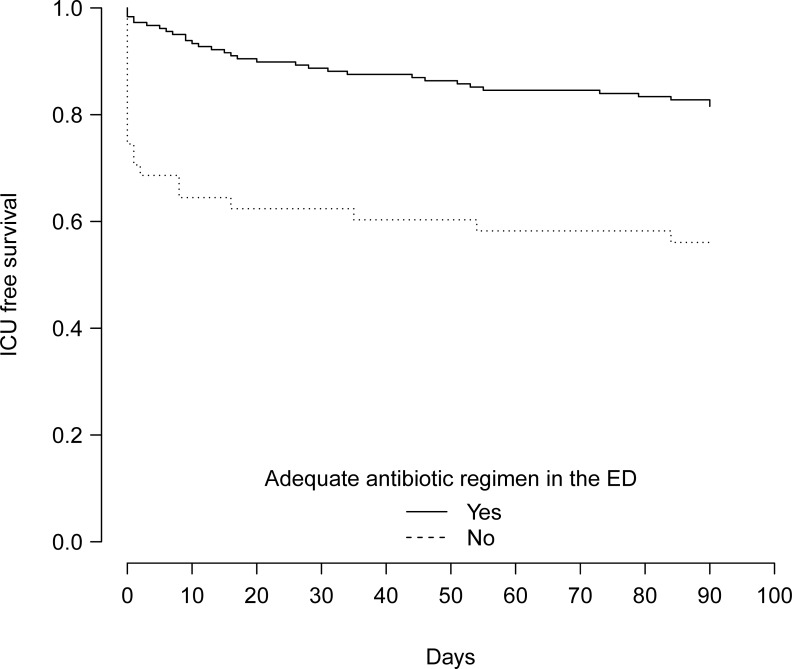
Results: We included 249 patients. Median age was 60 years and 67.9% had hematological malignancies, 26 (10.4%) were admitted to the ICU and 23 (9.8%) died during hospital stay. Among the 173 patients at low risk according to the MASCC risk-index, 56 (32.4%) presented at least one complication including 11 deaths. The MASCC risk-index had a sensitivity and a specificity of 0.78% and 0.43%, respectively, in predicting the absence of complication and the AUC was 0.67. The time to antibiotic initiation in the ED was not associated with the outcome after adjusting for performance status and shock-index. Conversely, an inadequate ED antibiotic regimen was associated with higher ICU admission or death during hospital stay (OR = 3.50; 95% CI = 1.49 to 8.28).
Conclusion: An inadequate ED antibiotic regimen in patients with FN was significantly associated with higher ICU admission or death during hospital stay.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Similar articles
-
Emergency department management of chemotherapy related febrile neutropenia: An opportunity to improve care.Am J Emerg Med. 2021 Dec;50:5-9. doi: 10.1016/j.ajem.2021.07.008. Epub 2021 Jul 9. Am J Emerg Med. 2021. PMID: 34265732
-
A comparison of ED and direct admission care of cancer patients with febrile neutropenia.Am J Emerg Med. 2015 Jul;33(7):966-9. doi: 10.1016/j.ajem.2015.04.028. Epub 2015 Apr 23. Am J Emerg Med. 2015. PMID: 25959844
-
Can Risk Stratification Tools Be Utilized to Safely Discharge Low-Risk Febrile Neutropenic Patients from the Emergency Department?J Emerg Med. 2023 Jan;64(1):111-118. doi: 10.1016/j.jemermed.2022.10.010. Epub 2023 Jan 12. J Emerg Med. 2023. PMID: 36641256
-
Accuracy of the Multinational Association of Supportive Care in Cancer (MASCC) and Clinical Index of Stable Febrile Neutropenia (CISNE) scores for predicting serious complications in adult patients with febrile neutropenia: A systematic review and meta-analysis.Crit Rev Oncol Hematol. 2020 May;149:102922. doi: 10.1016/j.critrevonc.2020.102922. Epub 2020 Mar 3. Crit Rev Oncol Hematol. 2020. PMID: 32244162
-
Outpatient management of febrile neutropenia associated with cancer chemotherapy: risk stratification and treatment review.Am J Health Syst Pharm. 2015 Apr 15;72(8):619-31. doi: 10.2146/ajhp140194. Am J Health Syst Pharm. 2015. PMID: 25825185 Review.
Cited by
-
Risk Factors for Infections, Antibiotic Therapy, and Its Impact on Cancer Therapy Outcomes for Patients with Solid Tumors.Life (Basel). 2021 Dec 11;11(12):1387. doi: 10.3390/life11121387. Life (Basel). 2021. PMID: 34947918 Free PMC article. Review.
-
Understanding and Managing Sepsis in Patients With Cancer in the Era of Antimicrobial Resistance.Front Med (Lausanne). 2021 Mar 31;8:636547. doi: 10.3389/fmed.2021.636547. eCollection 2021. Front Med (Lausanne). 2021. PMID: 33869250 Free PMC article. Review.
-
Clinical prediction models for febrile neutropenia and its outcomes: a systematic review.Support Care Cancer. 2025 Jun 4;33(7):537. doi: 10.1007/s00520-025-09562-y. Support Care Cancer. 2025. PMID: 40467900 Free PMC article.
-
Can We Lower the Burden of Antimicrobial Resistance (AMR) in Heavily Immunocompromised Patients? A Narrative Review and Call to Action.Infect Dis Ther. 2025 Aug 7. doi: 10.1007/s40121-025-01204-4. Online ahead of print. Infect Dis Ther. 2025. PMID: 40772992 Review.
-
High Rate of Inappropriate Antibiotics in Patients with Hematologic Malignancies and Pseudomonas aeruginosa Bacteremia following International Guideline Recommendations.Microbiol Spectr. 2023 Aug 17;11(4):e0067423. doi: 10.1128/spectrum.00674-23. Epub 2023 Jun 27. Microbiol Spectr. 2023. PMID: 37367629 Free PMC article.
References
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
