

Medication abortion use among low-income and rural Texans before and during state-imposed restrictions and after FDA-updated labeling
- PMID: 32109462
- PMCID: PMC8259503
- DOI: 10.1016/j.ajog.2020.02.028
Medication abortion use among low-income and rural Texans before and during state-imposed restrictions and after FDA-updated labeling
Abstract
Background: In 2013, the Texas legislature passed House Bill 2, restricting use of medication abortion to comply with Food and Drug Administration labeling from 2000. The Food and Drug Administration updated its labeling for medication abortion in 2016, alleviating some of the burdens imposed by House Bill 2.
Objective: Our objective was to identify the impact of House Bill 2 on medication abortion use by patient travel distance to an open clinic and income status.
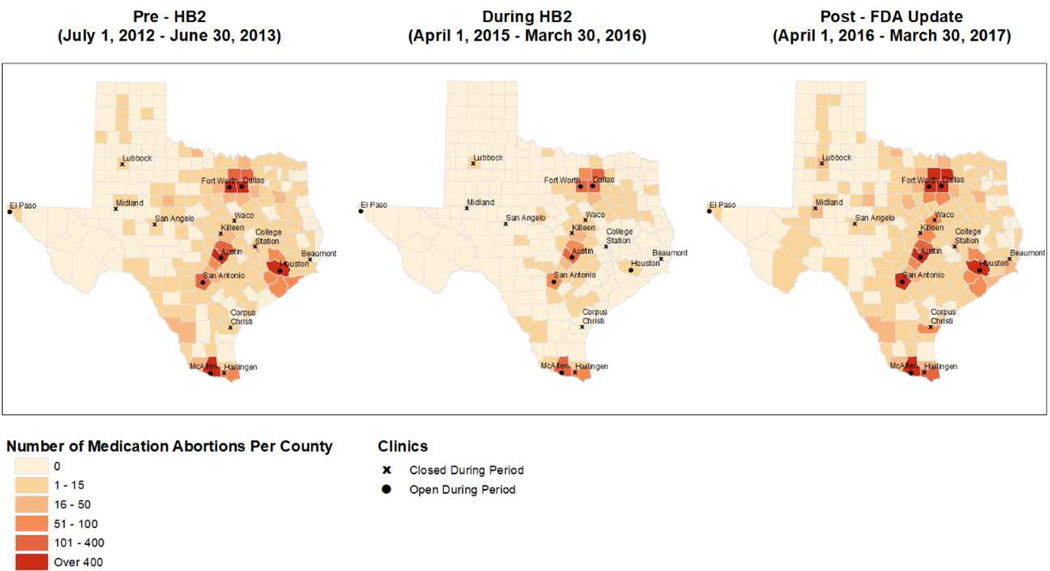
Materials and methods: In this retrospective study, we collected patient zip code, county of residence, type of abortion, family size, and income data on all patients who received an abortion (medication or aspiration) from 7 Texas abortion clinics in 3 time periods: pre-House Bill 2 (July 1, 2012-June 30, 2013), during House Bill 2 (April 1, 2015-March 30, 2016), and post-Food and Drug Administration labeling update (April 1, 2016-March 30, 2017). Patient driving distance to the clinic where care was obtained was categorized as 1-24, 25-49, 50-99, or 100+ miles. Patient county of residence was categorized by availability of a clinic during House Bill 2 (open clinic), county with a House Bill 2-related clinic closure (closed clinic), or no clinic any time period. Patient income was categorized as ≤110% federal poverty level (low-income) and >110% federal poverty level. Change in medication abortion use in the 3 time periods by patient driving distance, residence in a county with an open clinic, and income status were evaluated using χ2 tests and logistic regression. We used geospatial mapping to depict the spatial distribution of patients who obtained a medication abortion in each time period.
Results: Among 70,578 abortion procedures, medication abortion comprised 26%, 7%, and 29% of cases pre-House Bill 2, during House Bill 2, and post-Food and Drug Administration labeling update, respectively. During House Bill 2, patients traveling 100+ miles compared to 1- 24 miles were less likely to use medication abortion (odds ratio, 0.21; 95% confidence interval, 0.15, 0.30), as were low-income compared to higher-income patients (odds ratio, 0.76; 95% confidence interval, 0.68, 0.85), and low-income, distant patients (adjusted odds ratio, 0.14; 95% confidence interval, 0.08, 0.25). Similarly, post-Food and Drug Administration labeling update, rebound in medication abortion use was less pronounced for patients traveling 100+ miles compared to 1-24 miles (odds ratio, 0.82; 95% confidence interval, 0.74, 0.91), low-income compared to higher-income patients (odds ratio, 0.77; 95% confidence interval, 0.72, 0.81), and low-income, distant patients (adjusted odds ratio, 0.80; 95% confidence interval, 0.68, 0.94). Post-Food and Drug Administration labeling update, patients residing in counties with House Bill 2-related clinic closures were less likely to receive medication abortion as driving distance increased (52% traveling 25-49 miles, 41% traveling 50-99 miles, and 26% traveling 100+ miles, P < .05). Geospatial mapping demonstrated that patients traveled from all over the state to receive medication abortion pre-House Bill 2 and post-Food and Drug Administration labeling update, whereas during House Bill 2, only those living in or near a county with an open clinic obtained medication abortion.
Conclusion: Texas state law drastically restricted access to medication abortion and had a disproportionate impact on low-income patients and those living farther from an open clinic. After the Food and Drug Administration labeling update, medication abortion use rebounded, but disparities in use remained.
Keywords: Texas; United States; abortion rate; epidemiology; ethics; income; induced abortion; legislation; rural population; spatial analysis.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures

Similar articles
-
Rebound of medication abortion in Texas following updated mifepristone label.Contraception. 2019 May;99(5):278-280. doi: 10.1016/j.contraception.2019.01.001. Epub 2019 Jan 23. Contraception. 2019. PMID: 30684470 Free PMC article.
-
Impact of Clinic Closures on Women Obtaining Abortion Services After Implementation of a Restrictive Law in Texas.Am J Public Health. 2016 May;106(5):857-64. doi: 10.2105/AJPH.2016.303134. Epub 2016 Mar 17. Am J Public Health. 2016. PMID: 26985603 Free PMC article.
-
Differences in abortion rates by race-ethnicity after implementation of a restrictive Texas law.Contraception. 2020 Aug;102(2):109-114. doi: 10.1016/j.contraception.2020.04.008. Epub 2020 Apr 15. Contraception. 2020. PMID: 32304767 Free PMC article.
-
Update on medication abortion.J Midwifery Womens Health. 2007 Jan-Feb;52(1):23-30. doi: 10.1016/j.jmwh.2006.10.006. J Midwifery Womens Health. 2007. PMID: 17207747 Review.
-
Medical abortion offered in pharmacy versus clinic-based settings.Cochrane Database Syst Rev. 2021 Jun 11;6(6):CD013566. doi: 10.1002/14651858.CD013566.pub2. Cochrane Database Syst Rev. 2021. PMID: 34114643 Free PMC article.
Cited by
-
Comparing preference for and use of medication abortion in Texas after policy changes in 2014 and 2018.Contraception. 2023 Mar;119:109912. doi: 10.1016/j.contraception.2022.11.003. Epub 2022 Dec 5. Contraception. 2023. PMID: 36473511 Free PMC article.
-
Access to Abortion After Dobbs v. Jackson Women's Health Organization: Advocacy and a Call to Action for the Profession of Psychiatry.Acad Psychiatry. 2023 Feb;47(1):1-6. doi: 10.1007/s40596-022-01729-7. Acad Psychiatry. 2023. PMID: 36369427 Free PMC article. No abstract available.
References
-
- Jones RK, Boonstra H. The Public Health Implications of the FDA Update to the Medication Abortion Label. Guttmacher Institute; 2016.
-
- Medical management of first-trimester abortion. Contraception 2014;89:148–61. - PubMed
-
- Sheldon WR, Winikoff B. Mifepristone label laws and trends in use: recent experiences in four US states. Contraception 2015;92:182–5. - PubMed
-
- Mifeprex (mifepristone) Information. Silver Spring, MD: U.S. Food & Drug Administration, February 2018. Available at https://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforP.... Retrieved January 9, 2019.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
