

Negative Symptoms in Schizophrenia: A Review and Clinical Guide for Recognition, Assessment, and Treatment
- PMID: 32110026
- PMCID: PMC7041437
- DOI: 10.2147/NDT.S225643
Negative Symptoms in Schizophrenia: A Review and Clinical Guide for Recognition, Assessment, and Treatment
Abstract
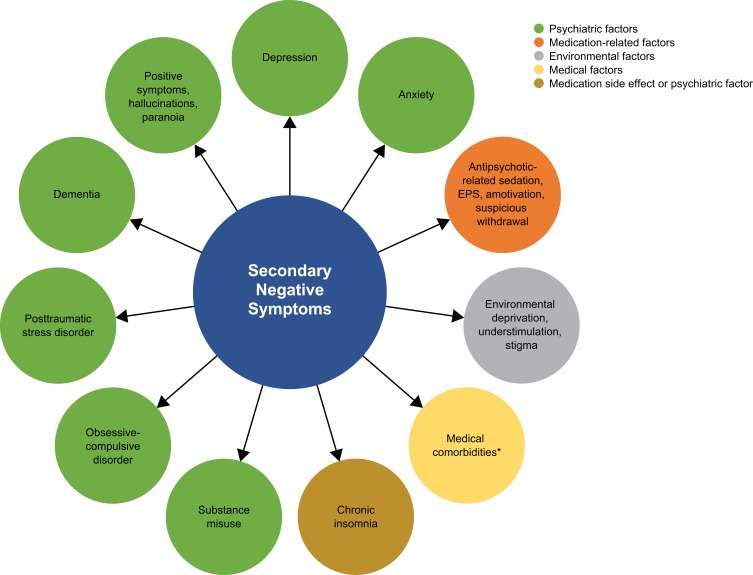
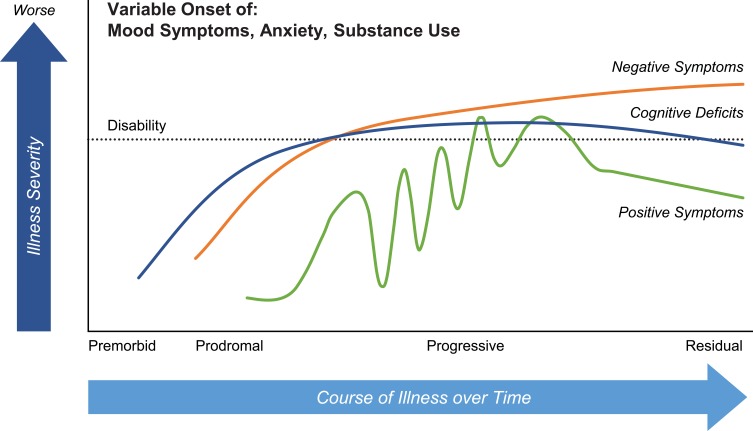
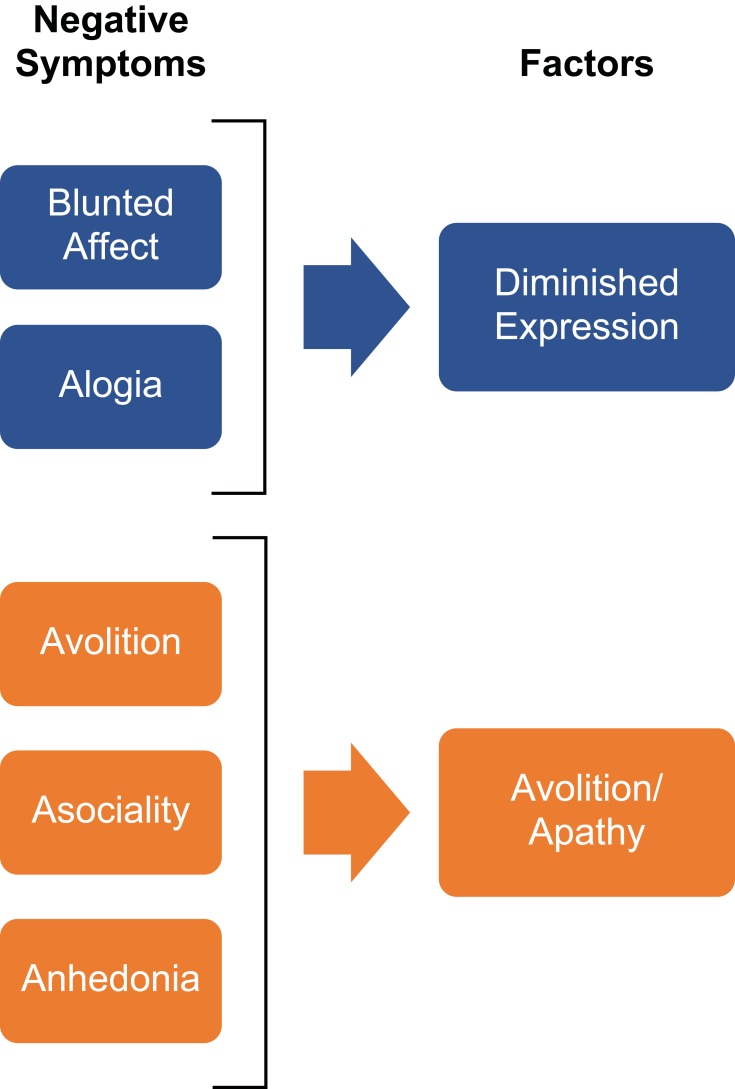
Schizophrenia is frequently a chronic and disabling disorder, characterized by heterogeneous positive and negative symptom constellations. The objective of this review was to provide information that may be useful for clinicians treating patients with negative symptoms of schizophrenia. Negative symptoms are a core component of schizophrenia that account for a large part of the long-term disability and poor functional outcomes in patients with the disorder. The term negative symptoms describes a lessening or absence of normal behaviors and functions related to motivation and interest, or verbal/emotional expression. The negative symptom domain consists of five key constructs: blunted affect, alogia (reduction in quantity of words spoken), avolition (reduced goal-directed activity due to decreased motivation), asociality, and anhedonia (reduced experience of pleasure). Negative symptoms are common in schizophrenia; up to 60% of patients may have prominent clinically relevant negative symptoms that require treatment. Negative symptoms can occur at any point in the course of illness, although they are reported as the most common first symptom of schizophrenia. Negative symptoms can be primary symptoms, which are intrinsic to the underlying pathophysiology of schizophrenia, or secondary symptoms that are related to psychiatric or medical comorbidities, adverse effects of treatment, or environmental factors. While secondary negative symptoms can improve as a consequence of treatment to improve symptoms in other domains (ie, positive symptoms, depressive symptoms or extrapyramidal symptoms), primary negative symptoms generally do not respond well to currently available antipsychotic treatment with dopamine D2 antagonists or partial D2 agonists. Since some patients may lack insight about the presence of negative symptoms, these are generally not the reason that patients seek clinical care, and clinicians should be especially vigilant for their presence. Negative symptoms clearly constitute an unmet medical need in schizophrenia, and new and effective treatments are urgently needed.
Keywords: clinical presentation; diagnosis; negative symptoms; prevalence; schizophrenia; treatment.
© 2020 Correll and Schooler.
Conflict of interest statement
Dr. Correll has been a consultant and/or advisor to or has received honoraria from: Alkermes, Allergan, Angelini, Boehringer-Ingelheim, Gedeon Richter, Gerson Lehrman Group, Indivior, IntraCellular Therapies, Janssen/J&J, LB Pharma, Lundbeck, MedAvante-ProPhase, Medscape, Merck, Neurocrine, Noven, Otsuka, Pfizer, Recordati, Rovi, Servier, Sumitomo Dainippon, Sunovion, Supernus, Takeda, and Teva. He has provided expert testimony for Bristol-Myers Squibb, Janssen, and Otsuka. He served on a Data Safety Monitoring Board for Boehringer-Ingelheim, Lundbeck, Rovi, Supernus, and Teva. He received royalties from UpToDate and grant support from Janssen and Takeda. He is also a shareholder of LB Pharma. Dr. Schooler has been a consultant and/or advisor to Alkermes, Allergan, GW Pharmaceuticals, IntraCellular Therapies, Lundbeck, Roche and Sunovion. She reports personal fees from Alkermes, Allergan, GW Pharmaceuticals, Intracellular Therapies, Lundbeck, Roche, Sunovion, and grants from Otsuka, outside the submitted work. The authors report no other conflicts of interest in this work.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
