

doi: 10.1016/j.joto.2019.06.001.
Epub 2019 Jul 3.
Transcanal endoscopic assisted skull base endolymphatic sac tumor resection: A rare disease with advanced technology
Affiliations
- PMID: 32110234
- PMCID: PMC7033593
- DOI: 10.1016/j.joto.2019.06.001
Item in Clipboard
Transcanal endoscopic assisted skull base endolymphatic sac tumor resection: A rare disease with advanced technology
J Otol.
2020 Mar.
Erratum in
-
Erratum regarding missing Declaration of Competing Interest statements in previously published articles.J Otol. 2020 Dec;15(4):180. doi: 10.1016/j.joto.2020.10.001. Epub 2020 Oct 13. J Otol. 2020. PMID: 33293924 Free PMC article.
Abstract
Endolymphatic sac tumors (ELSTs) are rare, papillary adenomatous tumors that arise from the endothelium of the endolymphatic sac. We demonstrate a difficult case of endolymphatic sac tumor and how it is managed via transcanal endoscopic assisted technique, with discussion of feasibility of transcanal approach to lateral skull base tumor.
Keywords: Endolymphatic sac; Lateral skull base; Transcanal combined endoscopic microscopic approach; Transcanal endoscopic assisted technique.
© 2019 PLA General Hospital Department of Otolaryngology Head and Neck Surgery. Production and hosting by Elsevier (Singapore) Pte Ltd.
Figures
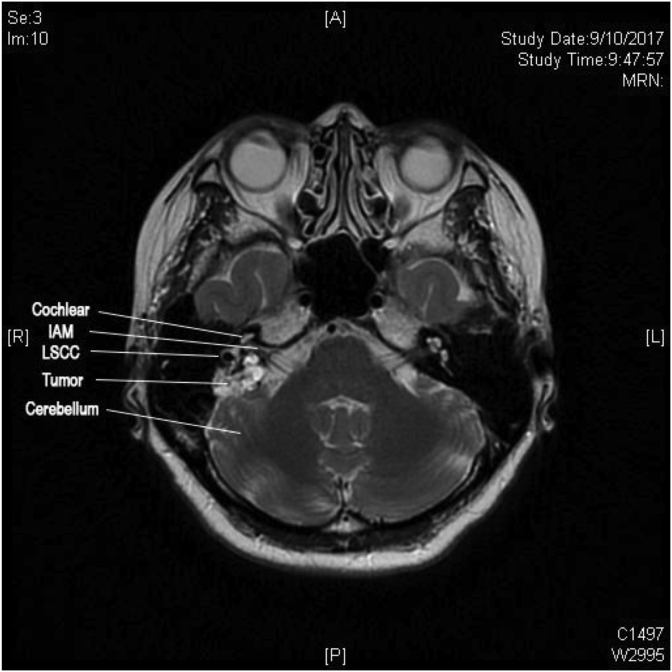
MRI showing pre-operative tumor involvement (IAM: Internal Acoustic meatus; LSCC: Lateral semicircular canal).
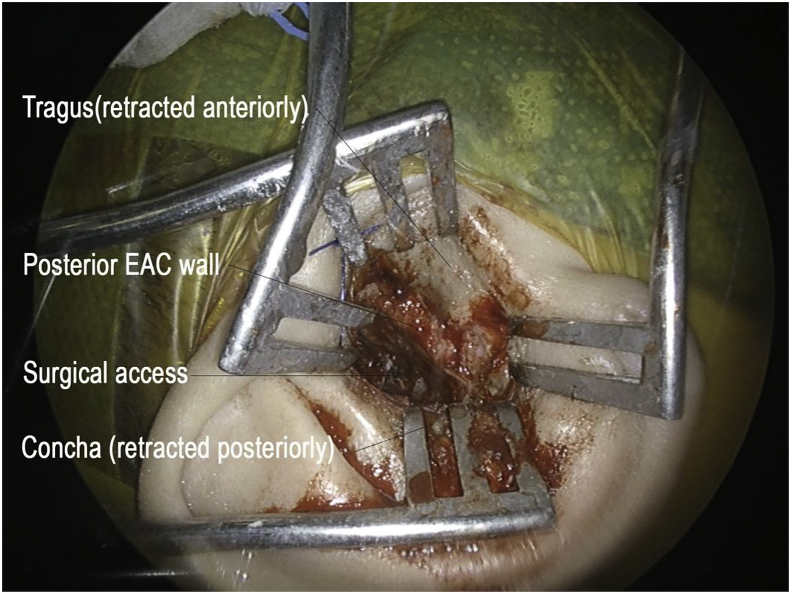
External incision of transcanal approach (EAC: External acoustic canal).
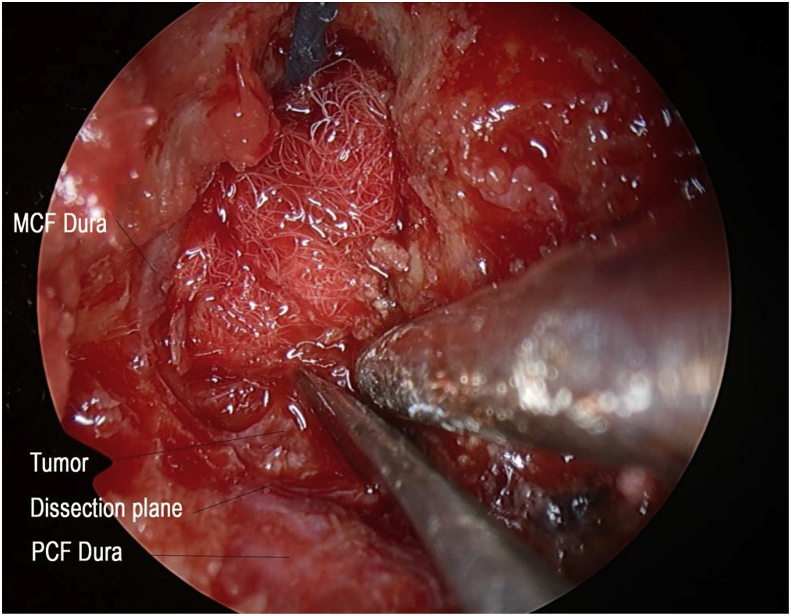
Tissue plane between tumor and dura with 4 K system (MCF: middle cranial fossa; PCF: posterior cranial fossa).
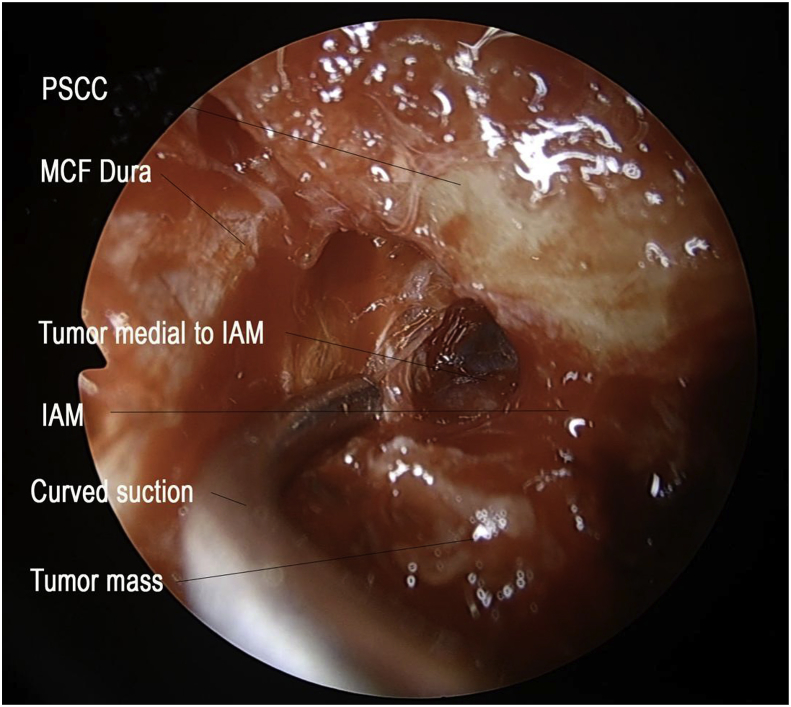
Endoscopic approach to Internal Acustic Meatus with curved instruments (PSCC: posterior semicircular canal; MCF: middle cranial fossa; IAM: internal acoustic meatus).
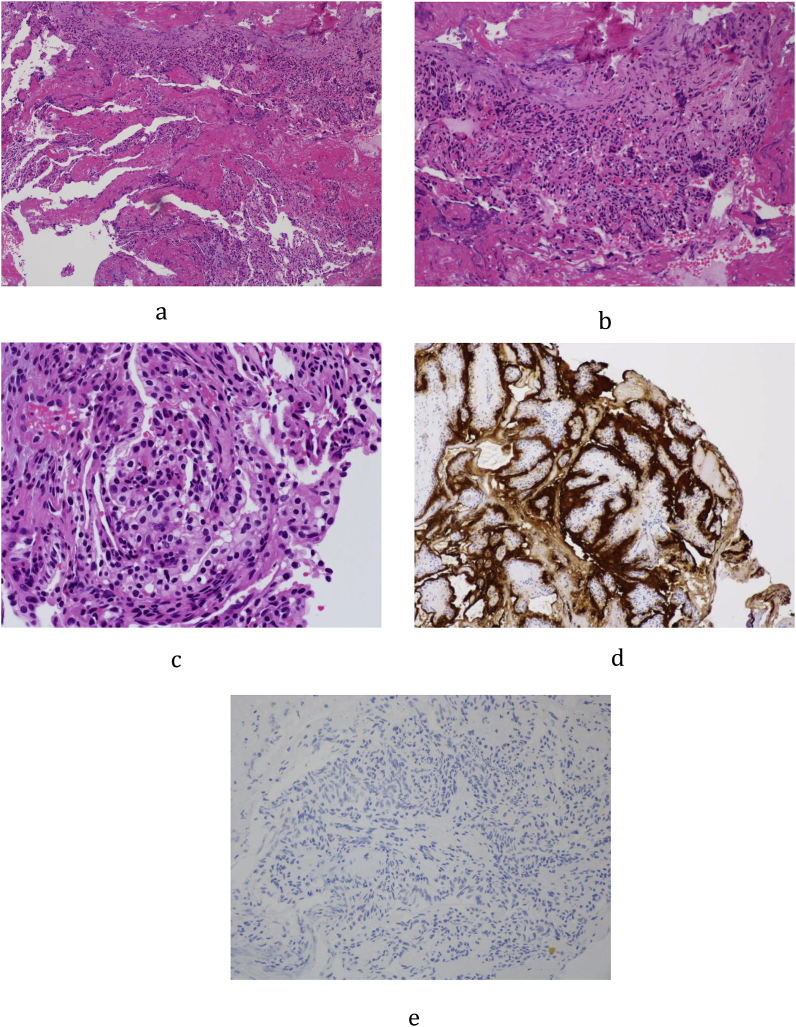
a: Low power magnification showing tumor fragments admixed both blood clot and fibrins. b: Higher power magnification showing papillary and glandular structures lined by a single layer of epithelium. c: High power magnification showing low grade nuclear features of tumor cells. d: Cytoderatin stain (AE1/AE3) highlights the lining cells. e: VHL stain were negative.
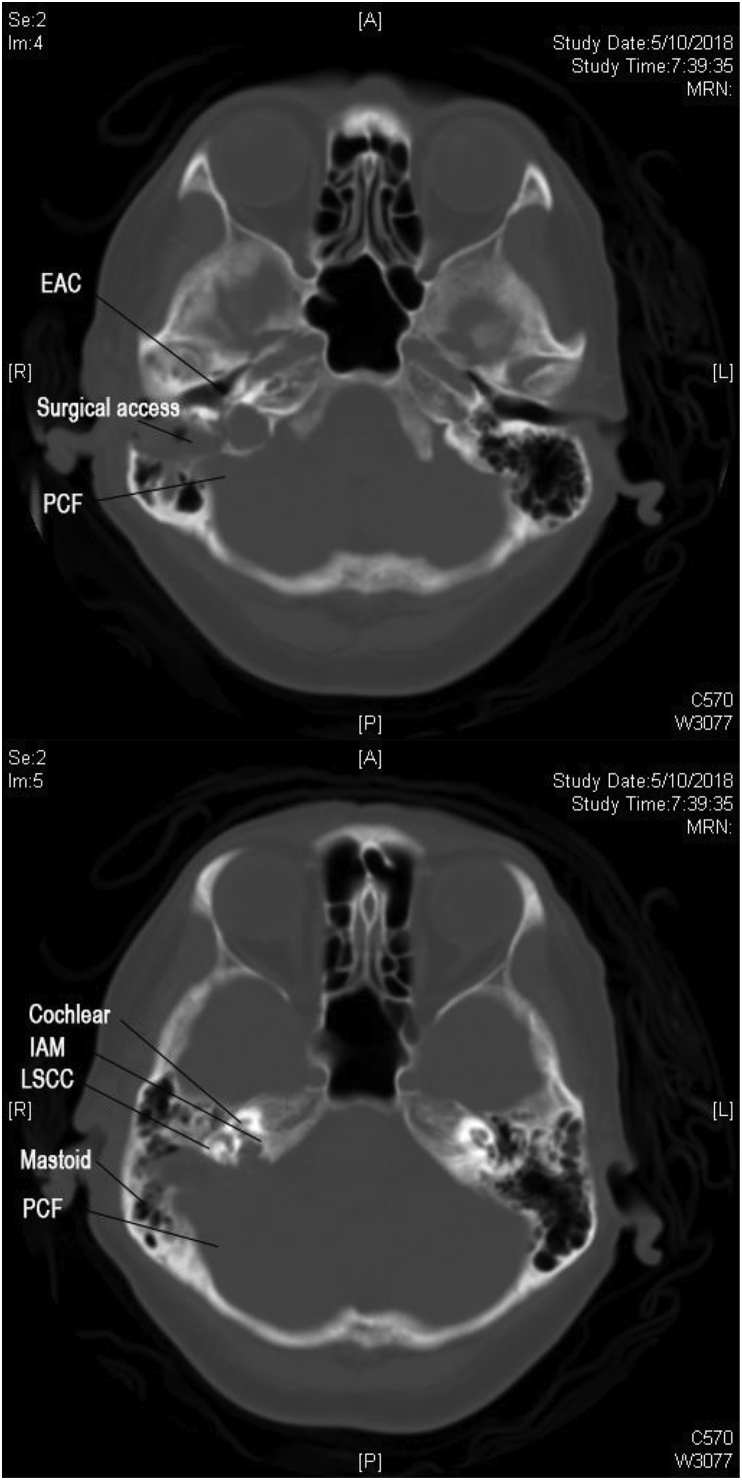
a,b: CT scan showing transcanal approach to Internal Acoustic Meatus and Jugular Bulb.
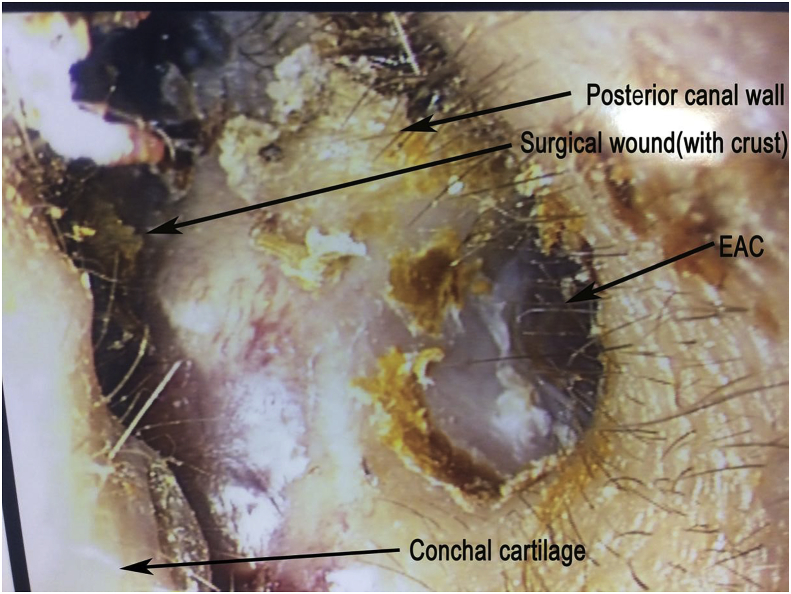
Intra-auricular wound, 2 weeks post op (EAC: External auditory canal).

Post operative 2 weeks external cosmetic appearance.
References
-
- Balasubramaniam S., Deshpande R.B., Misra B.K. Gamma knife radiosurgery in jugular foramen endolymphatic sac adenocarcinoma. J. Clin. Neurosci. 2009;16(5):710–711. - PubMed
-
- Bambakidis N.C., Megerian C.A., Ratcheson R.A. Differential grading of endolymphatic sac tumor extension by virtue of von Hippel-Lindau disease status. Otol. Neurotol. 2004;25(5):773–781. - PubMed
-
- Bell D., Gidley P., Levine N., Fuller G.N. Endolymphatic sac tumor (aggressive papillary tumor of middle ear and temporal bone): sine qua non radiology-pathology and the University of Texas MD Anderson Cancer Center experience. Ann. Diagn. Pathol. 2011;15(2):117–123. - PubMed
-
- Carlson M.L., Thom J.J., Driscoll C.L., Haynes D.S., Neff B.A., Link M.J., Wanna G.B. Management of primary and recurrent endolymphatic sac tumors. Otol. Neurotol. 2013;34(5):939–943. - PubMed
LinkOut - more resources
Full Text Sources
