

Getting started in endoscopic ear surgery
- PMID: 32110235
- PMCID: PMC7033523
- DOI: 10.1016/j.joto.2018.10.002
Getting started in endoscopic ear surgery
Erratum in
-
Erratum regarding missing Declaration of Competing Interest statements in previously published articles.J Otol. 2020 Dec;15(4):180. doi: 10.1016/j.joto.2020.10.001. Epub 2020 Oct 13. J Otol. 2020. PMID: 33293924 Free PMC article.
Abstract
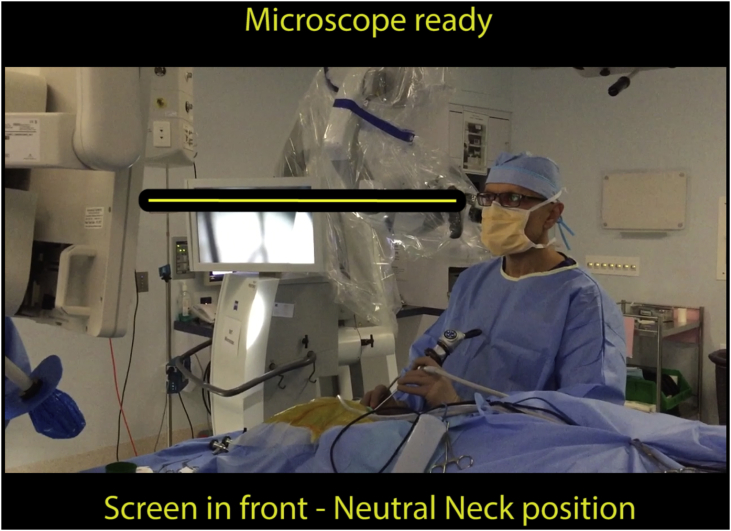
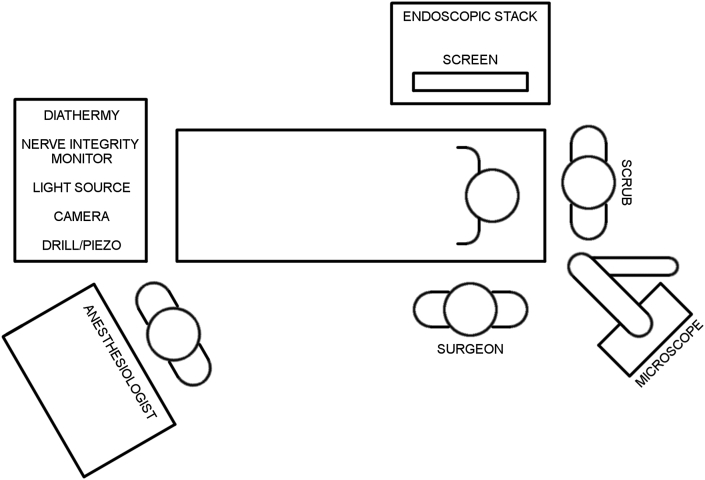
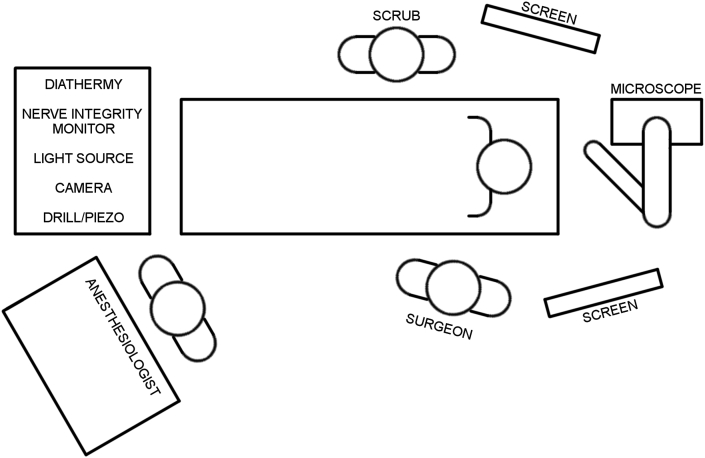
Endoscopic ear surgery (EES) is an exciting, rapidly developing and innovative field of otologic surgery. Technically and conceptually, EES is a significant departure from traditional microscopic transcanal approaches to the middle ear and canal that has shown very positive results with respect to patient outcomes. This review serves as a primer for the otologist and otology resident embarking on EES and discusses the theory surrounding the learning process, the optical chain for endoscopic surgery as well as other important underlying principles.
Keywords: Endoscopic; Endoscopic Ear Surgery; Optical Chain.
© 2018 PLA General Hospital Department of Otolaryngology Head and Neck Surgery. Production and hosting by Elsevier (Singapore) Pte Ltd.
Figures





References
-
- Berber E., Siperstein A.E. Understanding and optimizing laparoscopic videosystems. Surg. Endosc. 2001;15(8):781–787. - PubMed
-
- Berci G., Wren S.M., Stain S.C., Peters J., Paz-Partlow M. Individual assessment of visual perception by surgeons observing the same laparoscopic organs with various imaging systems. Surg. Endosc. 1995;9(9):967–973. - PubMed
-
- Bjork R.A. Memory and metamemory considerations in the training of human beings. In: Metcalfe J., Shimamura A., editors. Metacognition: Knowing about Knowing. MIT Press; Cambridge, MA: 1994. pp. 185–205.
-
- Brown S.I., White C., Wipat K., Hanna G.B., Frank T.G., Cuschieri A. Characterizing the "gold standard" image for laparoscopic surgery. Surg. Endosc. 2004;18(8):1192–1195. - PubMed
-
- Champagne C., Regloix S.B., Genestier L., Crambert A., Maurin O., Pons Y. Endoscopic septoplasty: learning curve. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2016;133(3):167–170. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
