

Fat Embolism, Fat Embolism Syndrome and the Autopsy
- PMID: 32110249
- PMCID: PMC6997986
- DOI: 10.1177/1925362119896351
Fat Embolism, Fat Embolism Syndrome and the Autopsy
Abstract
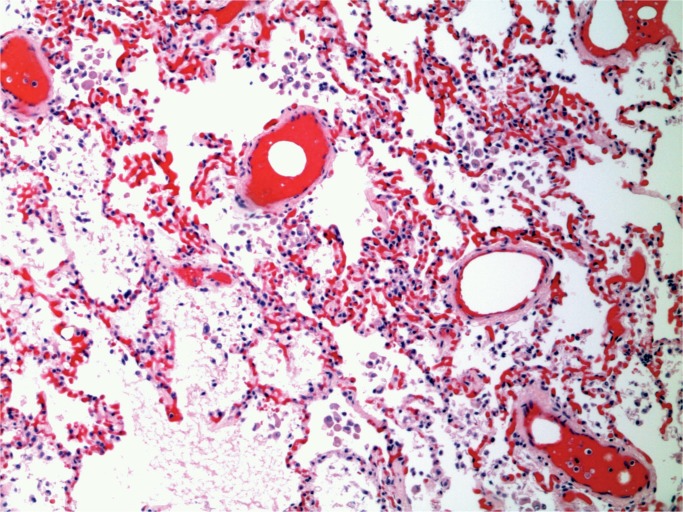
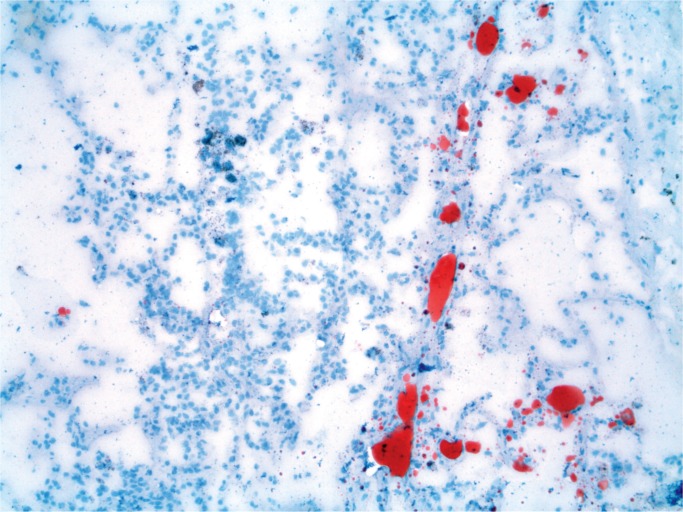
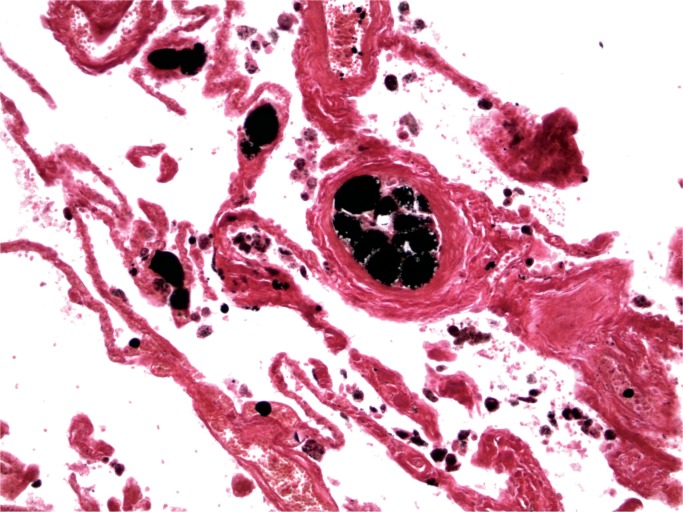
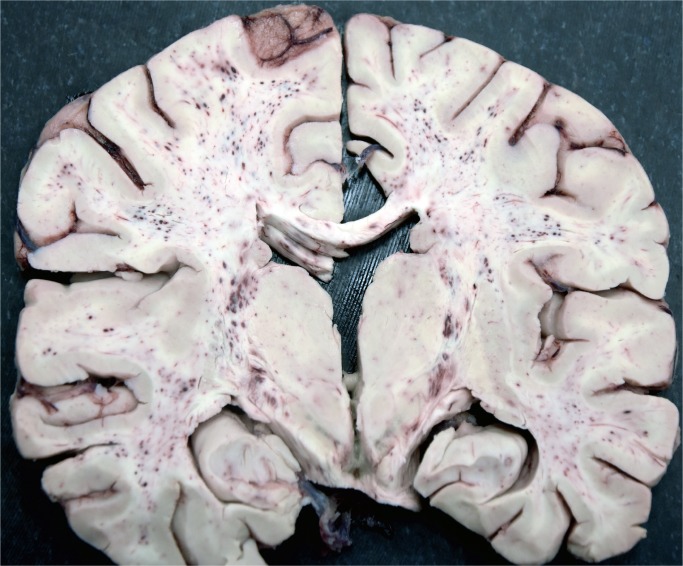
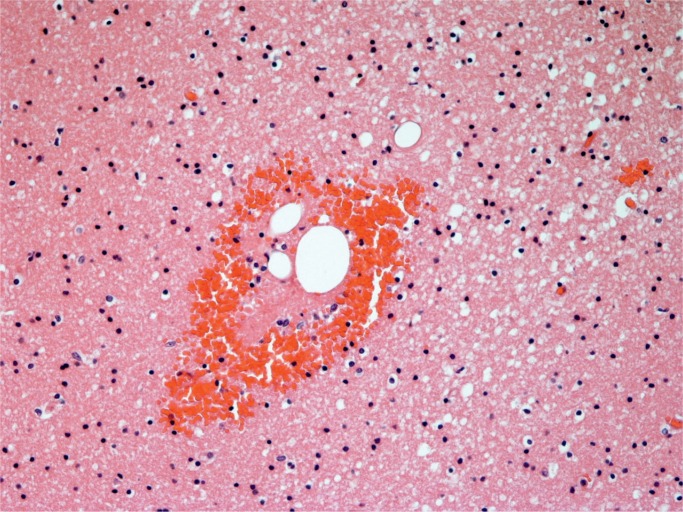
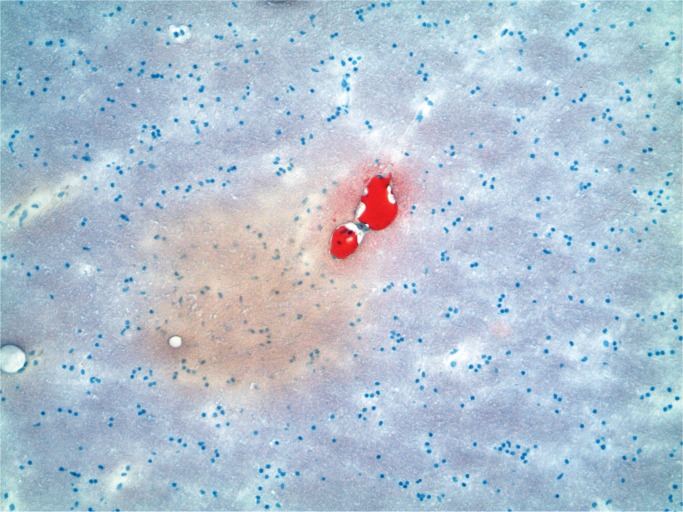
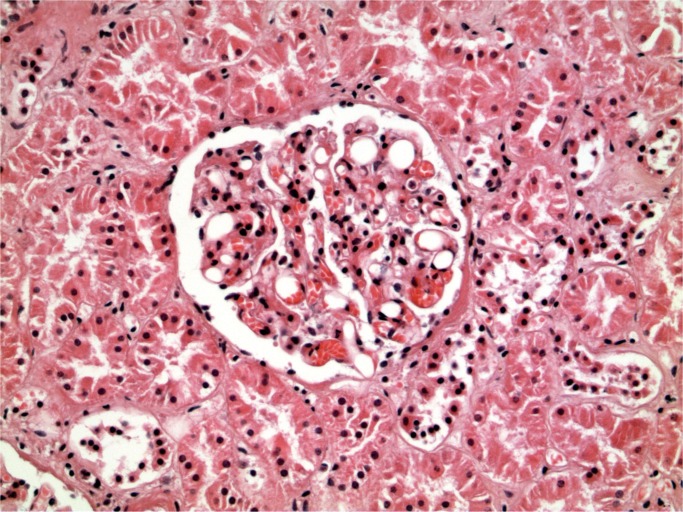
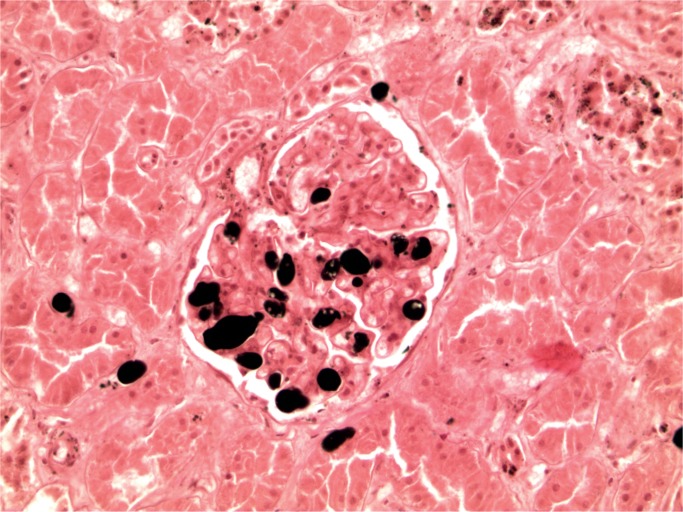
Fat embolism is common following trauma and is a common autopsy finding in these cases. It may also be seen in non-traumatic cases and is seen in children as well as adults. In comparison fat embolism syndrome (FES) only occurs in a small number of trauma and non-trauma cases. Clinical diagnosis is based on characteristic clinical and laboratory findings. Fat embolism exerts its effect by mechanical blockage of vessels and/or by biochemical means including breakdown of fat to free fatty acids causing an inflammatory response. Fat embolism can be identified at autopsy on microscopy of the lungs using fat stains conducted on frozen tissue, including on formalin fixed but not processed tissue. With FES fat emboli can be seen in other organs including the brain, kidney and myocardium. Fat can also be identified with post-fixation staining, typically with osmium tetroxide. Scoring systems have been developed to try and determine the severity of fat embolism in lung tissue. Fat embolism is also common following resuscitation. When no resuscitation has taken place, the presence of fat on lung histology has been used as proof of vitality. Diagnosis of fat embolism syndrome at autopsy requires analysis of the history, clinical and laboratory findings along with autopsy investigations to determine its relevance, but is an important diagnosis to make which is not always identified clinically. This paper reviews the history, clinical and laboratory findings and diagnosis of fat embolism and fat embolism syndrome at autopsy.
Keywords: Autopsy; Embolism; Fat; Forensic pathology; Microscopy; Syndrome.
© 2019 The Authors.
Conflict of interest statement
Disclosures & Declaration of Conflicts of Interest: The authors, reviewers, editors, and publication staff do not report any relevant conflicts of interest
Figures


References
-
- Lehman EP, McNattin RF. Fat embolism: II. Incidence at postmortem. Arch Surg. 1928. August; 17(2):179–89. 10.1001/archsurg.1928.01140080003001. - DOI
-
- Vance BM. The significance of fat embolism. Arch Surg. 1931. September; 23(3):426–65. 10.1001/archsurg.1931.01160090071002. - DOI
-
- Robb-Smith AH. Pulmonary fat-embolism. Lancet. 1941. February; 237(6127):135–41. 10.1016/s0140-6736(00)77494-0. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous