

The analgesic efficacy compared ultrasound-guided continuous transverse abdominis plane block with epidural analgesia following abdominal surgery: a systematic review and meta-analysis of randomized controlled trials
- PMID: 32111162
- PMCID: PMC7048149
- DOI: 10.1186/s12871-020-00969-0
The analgesic efficacy compared ultrasound-guided continuous transverse abdominis plane block with epidural analgesia following abdominal surgery: a systematic review and meta-analysis of randomized controlled trials
Abstract
Background: This review and meta-analysis aims to evaluate the analgesic efficacy of continuous transversus abdominis plane (TAP) block compared with epidural analgesia (EA) in adults after abdominal surgery.
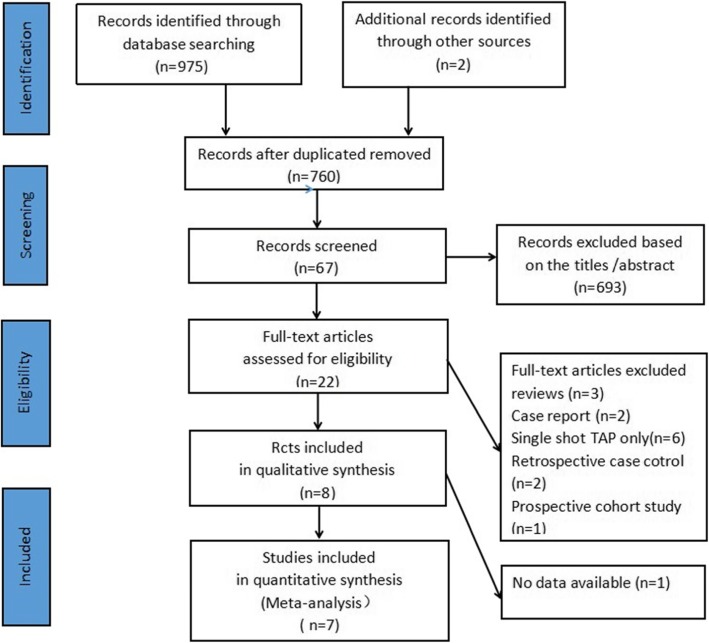
Methods: The databases PubMed, Embase and Cochrane Central Register were searched from inception to June 2019 for all available randomized controlled trials (RCTs) that evaluated the analgesic efficacy of continuous TAP block compared with EA after abdominal surgery. The weighted mean differences (WMDs) were estimates for continuous variables with a 95% confidence interval (CI) and risk ratio (RR) for dichotomous data. The pre-specified primary outcome was the dynamic pain scores 24 h postoperatively.
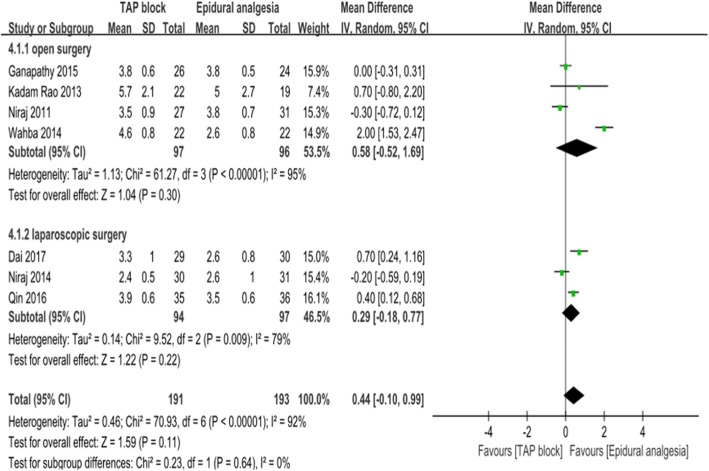
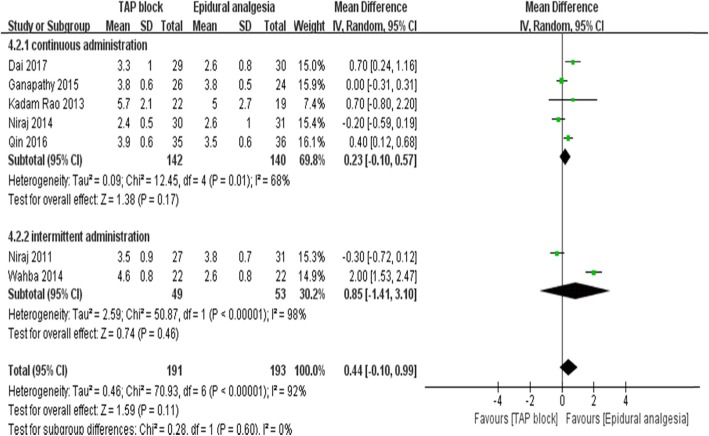
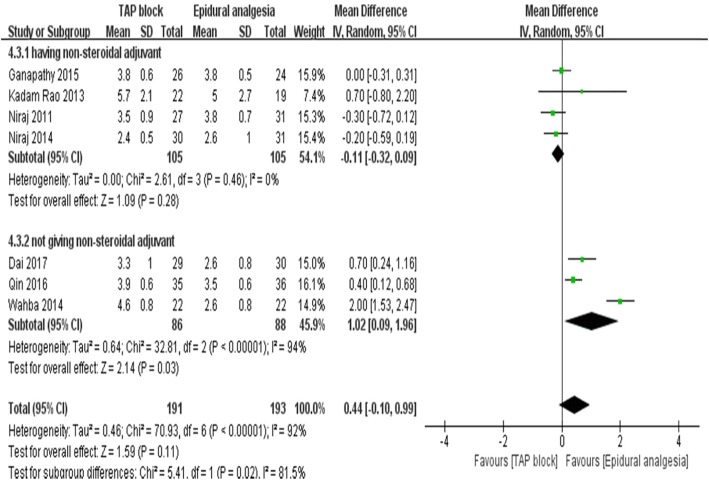
Results: Eight trials including 453 patients (TAP block:224 patients; EA: 229 patients) ultimately met the inclusion criteria and seven trials were included in the meta-analysis. Dynamic pain scores after 24 h were equivalent between TAP block and EA groups (WMD:0.44; 95% CI: 0.1 to 0.99; I2 = 91%; p = 0.11). The analysis showed a significant difference between the subgroups according to regularly administering (4 trials; WMD:-0.11; 95% CI: - 0.32 to 0.09; I2 = 0%; p = 0.28) non-steroidal anti-inflammatory drugs (NSAIDs) or not (3 trials; WMD:1.02; 95% CI: 0.09 to 1.96; I2 = 94%; p = 0.03) for adjuvant analgesics postoperatively. The measured time of the urinary catheter removal in the TAP group was significantly shorter (3 trials, WMD:-18.95, 95% CI:-25.22 to - 12.71; I2 = 0%; p < 0.01), as was time to first ambulation postoperatively (4 trials, WMD:-6.61, 95% CI: - 13.03 to - 0.19; I2 = 67%; p < 0.05).
Conclusion: Continuous TAP block, combined with NSAIDs, can provide non-inferior dynamic analgesia efficacy compared with EA in postoperative pain management after abdominal surgery. In addition, continuous TAP block is associated with fewer postoperative side effects.
Keywords: Abdominal surgery; Epidural analgesia; Meta-analysis; TAP block.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Popping DM, Elia N, Van Aken HK, et al. Impact of epidural analgesia on mortality and morbidity after surgery: systematic review and meta-analysis of randomized controlled trials. Ann Surg. 2014;259(6):1056–1067. - PubMed
-
- Bos EME, Hollmann MW, Lirk P. Safety and efficacy of epidural analgesia. Curr Opin Anaesthesiol. 2017;30(6):736–742. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
