

Factors associated with macrosomia, hypoglycaemia and low Apgar score among Fijian women with gestational diabetes mellitus
- PMID: 32111183
- PMCID: PMC7048039
- DOI: 10.1186/s12884-020-2821-6
Factors associated with macrosomia, hypoglycaemia and low Apgar score among Fijian women with gestational diabetes mellitus
Abstract
Background: Gestational diabetes mellitus (GDM) in Fiji is a serious public health issue. However, there are no recent studies on GDM among pregnant women in Fiji. The aim of this study was to examine prevalence of, and sociodemographic factors associated with adverse neonatal outcomes among Fijian women with GDM.
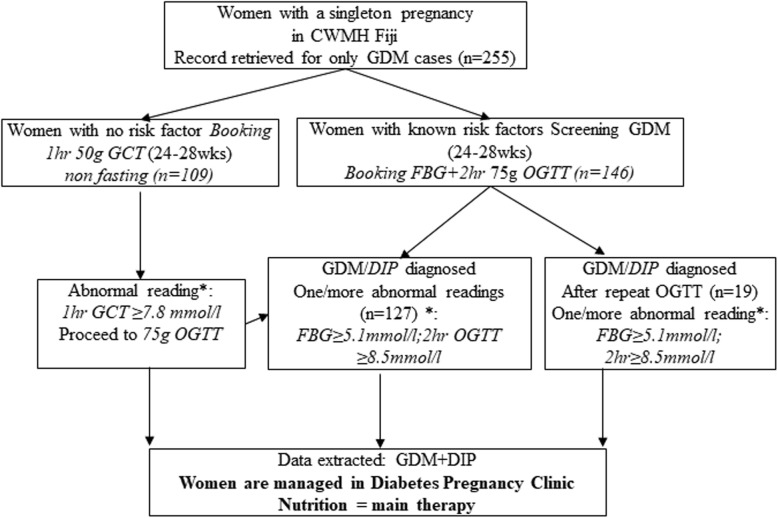
Methods: We used cross-sectional data of 255 pregnant women with GDM who gave birth to singleton infants at Colonial War Memorial Hospital (CWMH) in Suva city. Women underwent testing for GDM during antenatal clinic visits and were diagnosed using modified International Association of Diabetes and Pregnancy Study Groups (IADPSG) criteria. Multivariable logistic regression analysis was used to investigate factors associated with neonatal outcomes.
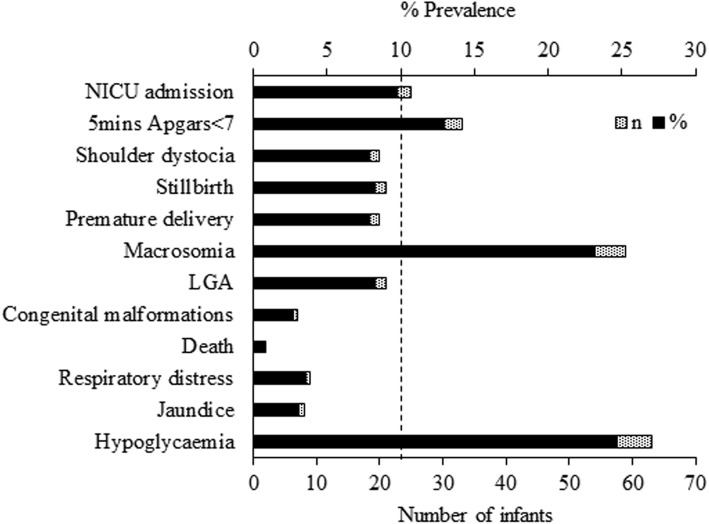
Results: Women with a previous baby weighing > 4 kg were 6.08 times more likely to experience neonatal macrosomia (Adjusted odds ratio (AOR) = 6.08; 95%CI: 2.46, 15.01). Compared to unmarried women, the odds of macrosomia among married women reduced by 71% (AOR = 0.29; 95%CI: 0.11, 0.77). Compared with delivery before 38 weeks of gestation, the infants of women who delivered between 38 and 41 weeks of gestation were 62 and 86% less likely to experience neonatal hypoglycaemia and Apgar score < 7 at 5 mins, respectively. The offspring of women who were overweight and obese had higher odds of neonatal hypoglycaemia. Late booking in gestation (≥28 weeks) was significantly associated with Apgar score < 7 at 5 min (AOR = 7.87; 95%CI: 1.11, 55.75). Maternal pre-eclampsia/pregnancy induced hypertension was another factor associated with low Apgar score in infants.
Conclusions: The study found high rates of adverse neonatal outcomes among off springs of Fijian women with GDM and showed that interventions targeting pregnant women who are overweight, had a previous baby weighing > 4 kg, had pre-eclampsia, delivered before 38 weeks of gestation, and those who booked later than 13 weeks in gestation, are needed to improve pregnancy outcomes.
Keywords: Apgar score; Diabetes; Fiji; Gestational diabetes mellitus (GDM); Hypoglycaemia; Macrosomia; Pacific people; Pregnancy.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
ATLANTIC DIP: Insulin Therapy for Women With IADPSG-Diagnosed Gestational Diabetes Mellitus. Does It Work?J Clin Endocrinol Metab. 2017 Mar 1;102(3):849-857. doi: 10.1210/jc.2016-2911. J Clin Endocrinol Metab. 2017. PMID: 27901638
-
Adverse Maternal Outcomes of Fijian Women with Gestational Diabetes Mellitus and the Associated Risk Factors.Reprod Sci. 2020 Nov;27(11):2029-2037. doi: 10.1007/s43032-020-00222-6. Epub 2020 Jun 16. Reprod Sci. 2020. PMID: 32548804
-
Obstetric and perinatal outcomes of singleton pregnancies conceived via assisted reproductive technology complicated by gestational diabetes mellitus: a prospective cohort study.BMC Pregnancy Childbirth. 2018 Dec 14;18(1):495. doi: 10.1186/s12884-018-2115-4. BMC Pregnancy Childbirth. 2018. PMID: 30547777 Free PMC article.
-
Association between gestational diabetes mellitus diagnostic criteria and adverse pregnancy outcomes-a systematic review and meta-analysis of adjusted effect sizes from studies using current diagnostic criteria.BMJ Open. 2024 Nov 21;14(11):e091258. doi: 10.1136/bmjopen-2024-091258. BMJ Open. 2024. PMID: 39578035 Free PMC article.
-
Effect of Different Types of Diagnostic Criteria for Gestational Diabetes Mellitus on Adverse Neonatal Outcomes: A Systematic Review, Meta-Analysis, and Meta-Regression.Diabetes Metab J. 2022 Jul;46(4):605-619. doi: 10.4093/dmj.2021.0178. Epub 2022 Mar 8. Diabetes Metab J. 2022. PMID: 35255550 Free PMC article.
Cited by
-
Refining the diagnosis of gestational diabetes mellitus: a systematic review and meta-analysis.Commun Med (Lond). 2023 Dec 18;3(1):185. doi: 10.1038/s43856-023-00393-8. Commun Med (Lond). 2023. PMID: 38110524 Free PMC article.
-
Establishment of a nomogram model to predict macrosomia in pregnant women with gestational diabetes mellitus.BMC Pregnancy Childbirth. 2021 Aug 22;21(1):581. doi: 10.1186/s12884-021-04049-0. BMC Pregnancy Childbirth. 2021. PMID: 34420518 Free PMC article.
-
The combination of symphysis-fundal height and abdominal circumference as a novel predictor of macrosomia in GDM and normal pregnancy.BMC Pregnancy Childbirth. 2020 Aug 12;20(1):461. doi: 10.1186/s12884-020-03157-7. BMC Pregnancy Childbirth. 2020. PMID: 32787792 Free PMC article.
-
Gestational diabetes and its effect on fetal thymus size: a case-control study.BMC Pregnancy Childbirth. 2025 Mar 21;25(1):330. doi: 10.1186/s12884-025-07468-5. BMC Pregnancy Childbirth. 2025. PMID: 40119297 Free PMC article.
-
Antenatal health and perinatal outcomes of Pacific Islander women in Australia with and without gestational diabetes: A ten-year retrospective cohort study.Aust N Z J Obstet Gynaecol. 2024 Oct;64(5):494-500. doi: 10.1111/ajo.13826. Epub 2024 Apr 25. Aust N Z J Obstet Gynaecol. 2024. PMID: 38661099 Free PMC article.
References
-
- Nankervis A, McIntyre H, Moses R, Ross G, Callaway L, Porter C, Jeffries W, Boorman C, De Vries B, AJMJ ME. ADIPS consensus guidelines for the testing and diagnosis of gestational diabetes mellitus in Australia. 2014.
-
- Simmons D. Epidemiology of diabetes in pregnancy. A Practical Manual of Diabetes in Pregnancy. 2017;3:1–16.
-
- Sellers EA, Dean HJ, Shafer LA, Martens PJ, Phillips-Beck W, Heaman M, Prior HJ, Dart AB, McGavock J, Morris M, et al. Exposure to gestational diabetes mellitus: impact on the development of early-onset type 2 diabetes in Canadian first nations and non-first nations offspring. Diabetes Care. 2016;39(12):2240–2246. doi: 10.2337/dc16-1148. - DOI - PubMed
-
- Dabelea D, Mayer-Davis EJ, Lamichhane AP, D'Agostino RB, Jr, Liese AD, Vehik KS, Narayan KM, Zeitler P, Hamman RF. Association of intrauterine exposure to maternal diabetes and obesity with type 2 diabetes in youth: the SEARCH case-control study. Diabetes Care. 2008;31(7):1422–1426. doi: 10.2337/dc07-2417. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
