

Comprehensive characterization of cell-free tumor DNA in plasma and urine of patients with renal tumors
- PMID: 32111235
- PMCID: PMC7048087
- DOI: 10.1186/s13073-020-00723-8
Comprehensive characterization of cell-free tumor DNA in plasma and urine of patients with renal tumors
Abstract
Background: Cell-free tumor-derived DNA (ctDNA) allows non-invasive monitoring of cancers, but its utility in renal cell cancer (RCC) has not been established.
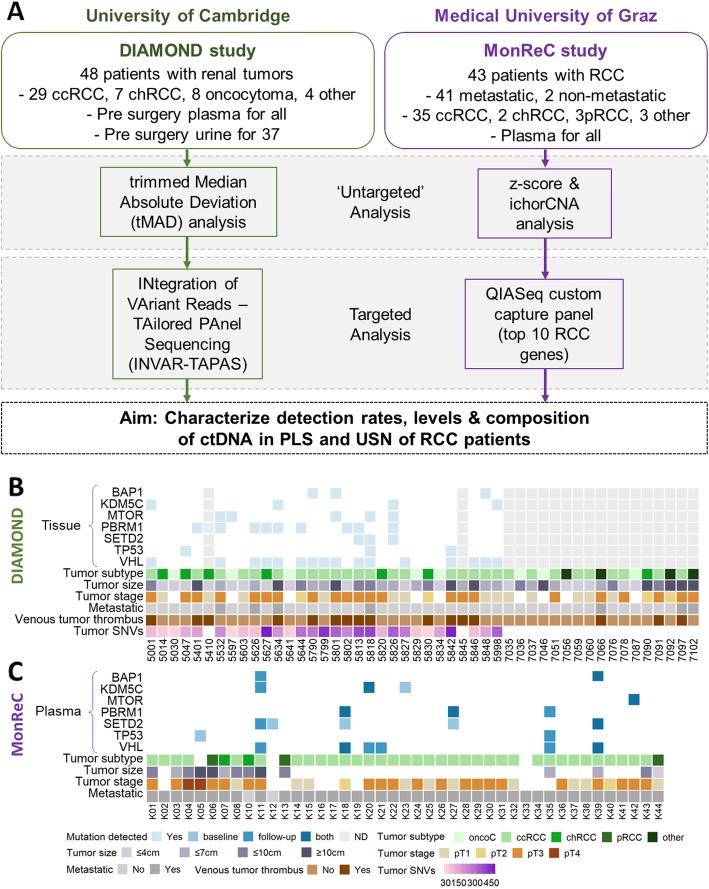
Methods: Here, a combination of untargeted and targeted sequencing methods, applied to two independent cohorts of patients (n = 91) with various renal tumor subtypes, were used to determine ctDNA content in plasma and urine.
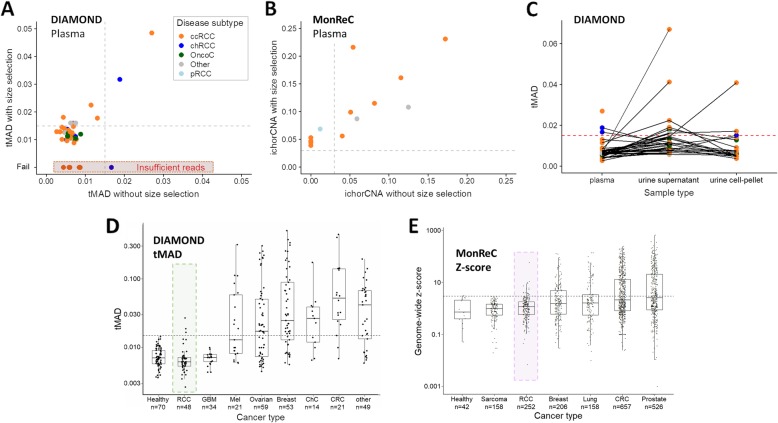
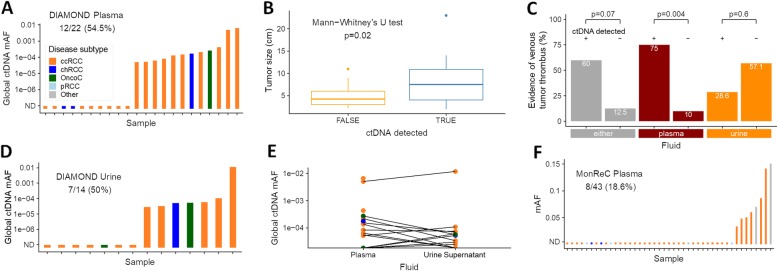
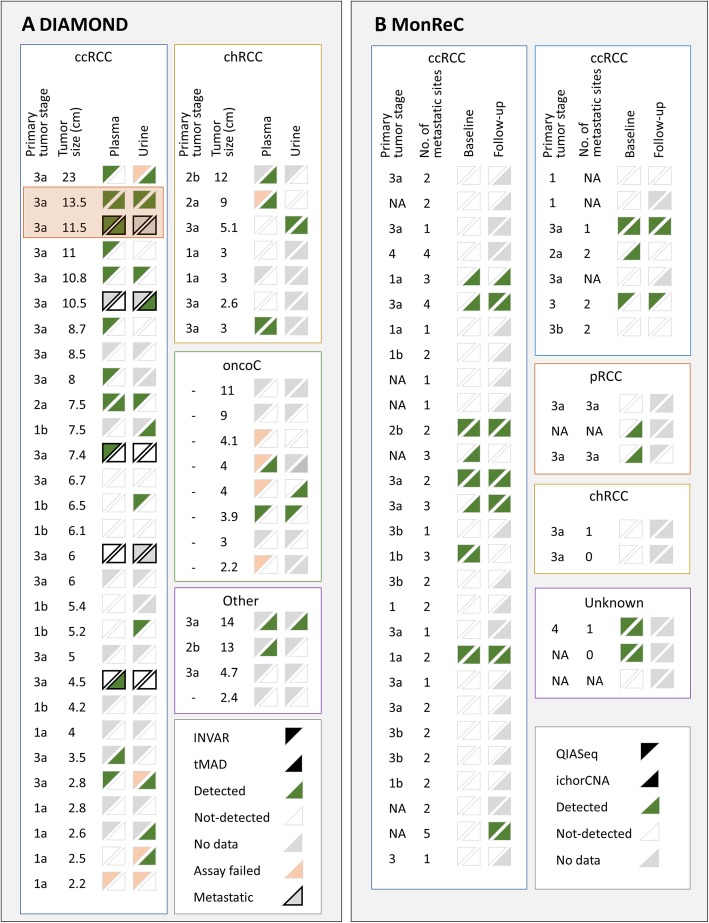
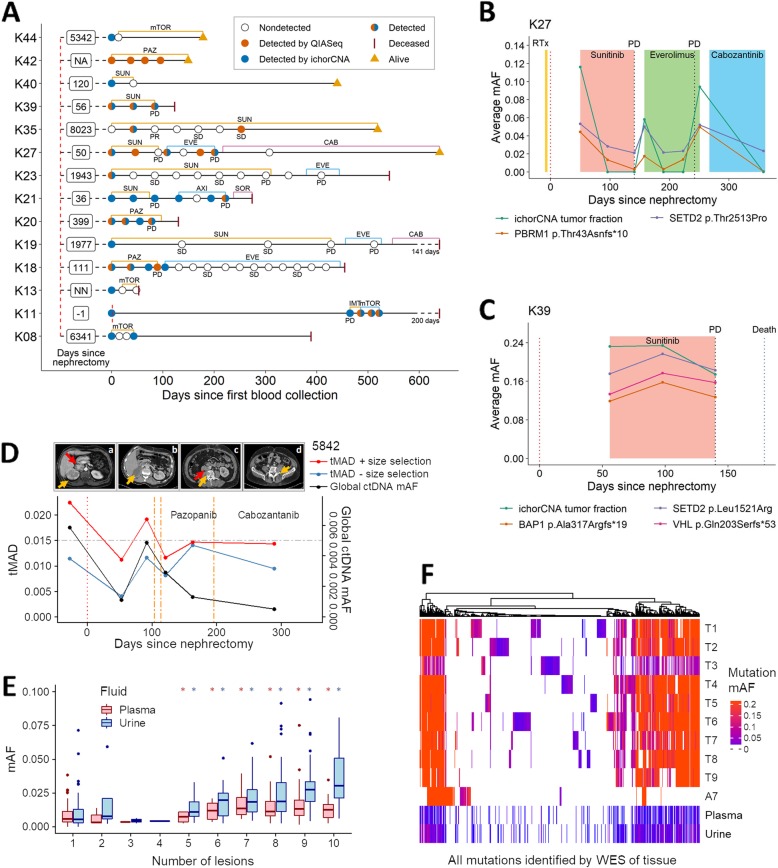
Results: Our data revealed lower plasma ctDNA levels in RCC relative to other cancers of similar size and stage, with untargeted detection in 27.5% of patients from both cohorts. A sensitive personalized approach, applied to plasma and urine from select patients (n = 22) improved detection to ~ 50%, including in patients with early-stage disease and even benign lesions. Detection in plasma, but not urine, was more frequent amongst patients with larger tumors and in those patients with venous tumor thrombus. With data from one extensively characterized patient, we observed that plasma and, for the first time, urine ctDNA may better represent tumor heterogeneity than a single tissue biopsy. Furthermore, in a subset of patients (n = 16), longitudinal sampling revealed that ctDNA can track disease course and may pre-empt radiological identification of minimal residual disease or disease progression on systemic therapy. Additional datasets will be required to validate these findings.
Conclusions: These data highlight RCC as a ctDNA-low malignancy. The biological reasons for this are yet to be determined. Nonetheless, our findings indicate potential clinical utility in the management of patients with renal tumors, provided improvement in isolation and detection approaches.
Keywords: Cell-free tumor DNA (ctDNA); Heterogeneity; Personalized analysis; Predictive biomarker; Renal cancer.
Conflict of interest statement
GDS has received educational grants from Pfizer, AstraZeneca, and Intuitive Surgical, consultancy fees from Merck, Pfizer, EUSA Pharma, and CMR Surgical, travel expenses from Pfizer and speaker fees from Pfizer. NR is a cofounder and shareholder of Inivata Ltd., a cancer genomics company that commercializes ctDNA analysis. TE and AM are employees of AstraZeneca and TE has received research support from AstraZeneca, Bayer, and Pfizer. Inivata and AstraZeneca had no role in the conceptualization, study design, data collection, and analysis, decision to publish, or preparation of the manuscript. Cancer Research UK has filed patent applications protecting methods described in this manuscript. CGS, FM, KH, JCMW, CEM, NR, and other authors may be listed as co-inventors on patent application numbers 1803596.4 (“Improvements in variant detection”), 1818159.4 (“Enhanced detection of target DNA by fragment size analysis”), and other potential patents describing methods for the analysis of DNA fragments and applications of ctDNA. EH receives funds for the Christian Doppler Laboratory for Liquid Biopsies for Early Detection of Cancer from Freenome and PreAnalytiX. The remaining authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
