

Use of thiazide diuretics for the prevention of recurrent kidney calculi: a systematic review and meta-analysis
- PMID: 32111248
- PMCID: PMC7048029
- DOI: 10.1186/s12967-020-02270-7
Use of thiazide diuretics for the prevention of recurrent kidney calculi: a systematic review and meta-analysis
Abstract
Background: Thiazide diuretics reduce the risk of recurrent kidney calculi in patients with kidney calculi or hypercalciuria. However, whether thiazide diuretics can definitely prevent recurrent kidney calculi remains unclear. We aimed to evaluate the effect and safety of thiazide diuretics on recurrent kidney calculi.
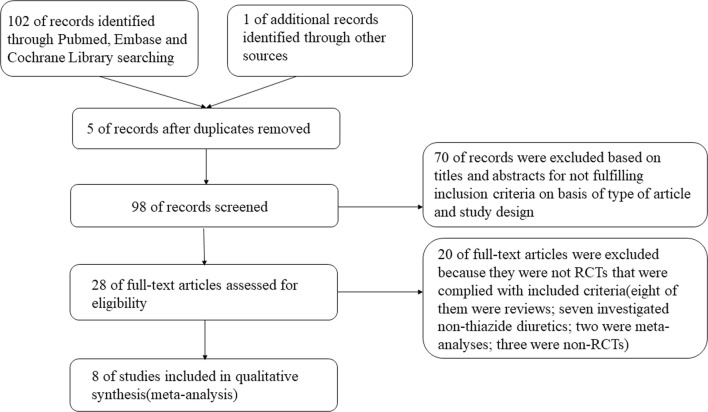
Methods: The PubMed, Cochrane Library, and EMBASE databases were systematically searched using the keywords thiazide diuretics and kidney calculi to identify randomized controlled trials (RCTs). The primary outcome was the incidence of recurrent kidney calculi, and the secondary outcome was the 24-h urinary calcium level. The pooled risk ratio (RR), risk difference (RD), standardized mean difference (SMD), and 95% confidence interval (CI) were calculated. The evidence quality was graded using the GRADE criteria, and recommendations for recurrent kidney calculus prevention using thiazide diuretics were reassessed.
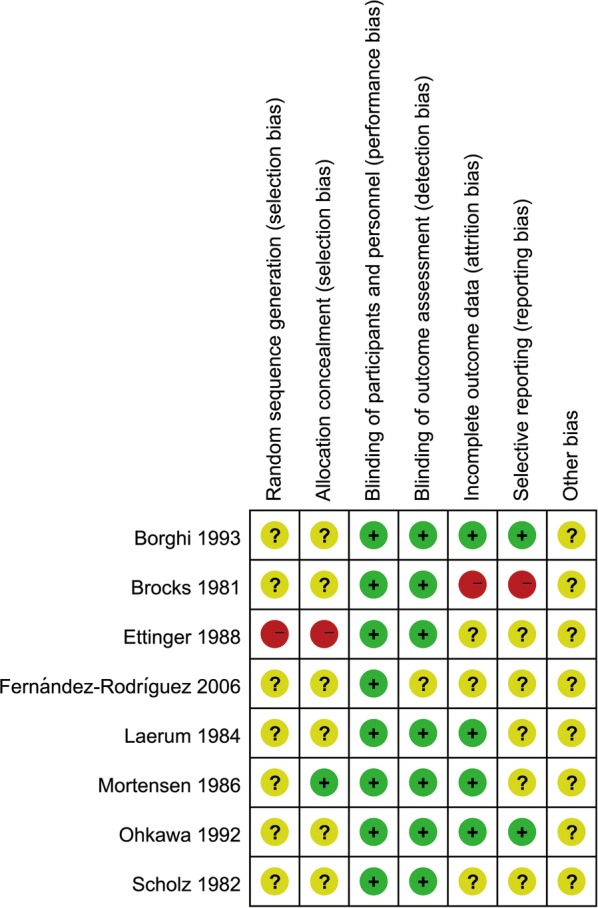
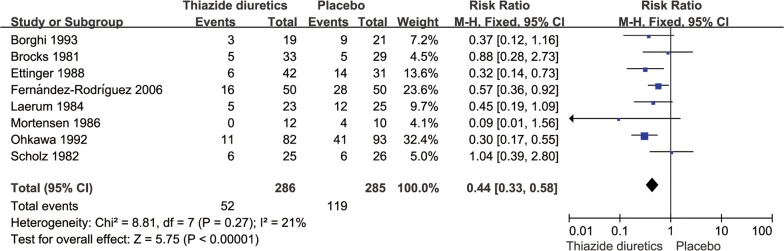
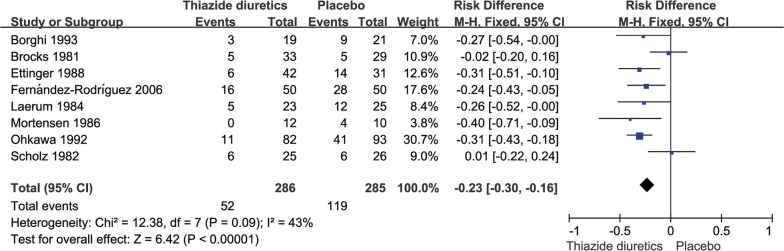
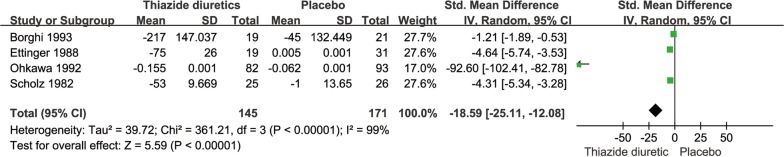
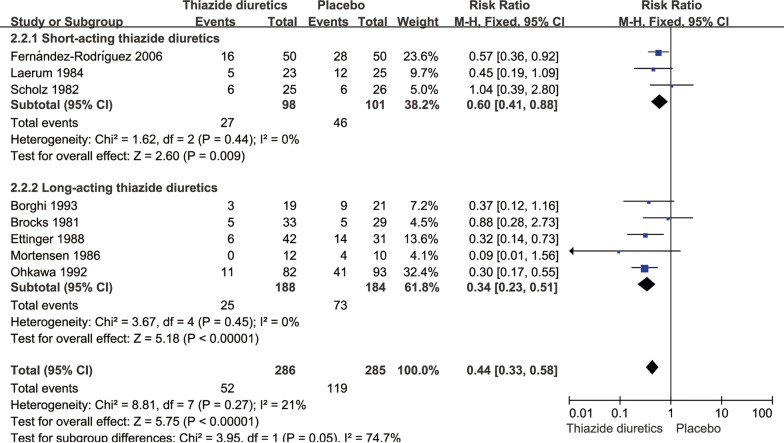
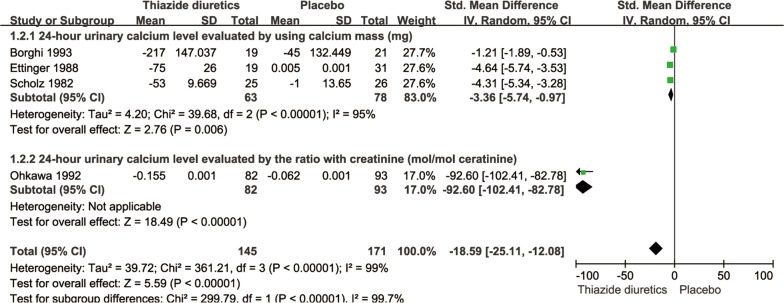
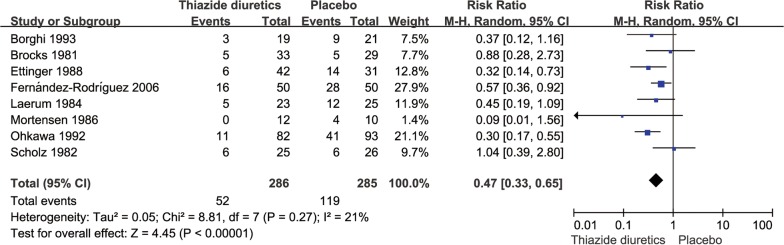
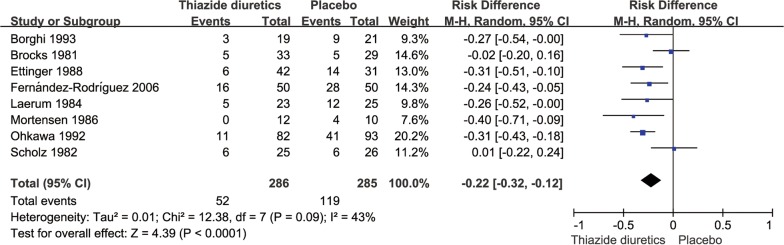
Results: Eight RCTs involving 571 patients were included. The pooled RR for the incidence of kidney calculi in the thiazide diuretic groups was 0.44 (95% CI 0.33-0.58, P < 0.0001) compared to that in the placebo and untreated groups; the pooled RD was - 0.23 (95% CI - 0.30 to - 0.16, P < 0.0001). The pooled SMD for the 24-h urinary calcium level was - 18.59 (95% CI - 25.11 to - 12.08, P < 0.0001). The thiazide diuretic groups had a high incidence of adverse reactions and low tolerance. The evidence quality for decrease in kidney calculus incidence using thiazide diuretics was low, while that for the 24-h urinary calcium level decrease among those with recurrent kidney calculi was moderate, and that for the decrease in kidney calculus incidence using short-acting and long-acting thiazide diuretics was low. The overall strength of recommendation for prevention of recurrent renal calculi using thiazide diuretics was not recommended. The subgroup and sensitivity analysis findings were robust.
Conclusions: Long-term use of thiazide diuretics reduces the incidence of recurrent renal calculi and 24-h urinary calcium level. However, the benefits are insufficient, and the evidence quality is low. Considering the adverse effects, poor patient compliance, and economic burden of long-term medication, their use in preventing recurrent kidney calculi is not recommended.
Keywords: Kidney calculi; Placebo; Randomized controlled trial; Thiazide diuretics.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Qaseem A, Dallas P, Forciea MA, Starkey M, Denberg TD, Clinical Guidelines Committee of the American College of P Dietary and pharmacologic management to prevent recurrent nephrolithiasis in adults: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2014;161:659–667. doi: 10.7326/M13-2908. - DOI - PubMed
-
- Cheungpasitporn W, Rossetti S, Friend K, Erickson SB, Lieske JC. Treatment effect, adherence, and safety of high fluid intake for the prevention of incident and recurrent kidney stones: a systematic review and meta-analysis. J Nephrol. 2016;29:211–219. doi: 10.1007/s40620-015-0210-4. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
