

Impact of point-of-care panel tests in ambulatory care: a systematic review and meta-analysis
- PMID: 32111610
- PMCID: PMC7050348
- DOI: 10.1136/bmjopen-2019-032132
Impact of point-of-care panel tests in ambulatory care: a systematic review and meta-analysis
Abstract
Objectives: This article summarises all the available evidence on the impact of introducing blood-based point-of-care panel testing (POCT) in ambulatory care on patient outcomes and healthcare processes.
Design: Systematic review and meta-analysis of randomised-controlled trials and before-after studies.
Data sources: Ovid Medline, Embase, Cochrane Database of Systematic Reviews, Cochrane CENTRAL, Database of Abstracts of Reviews and Effects, Science Citation Index from inception to 22 October 2019.
Eligibility criteria for selecting studies: Included studies were based in ambulatory care and compared POCT with laboratory testing. The primary outcome was the time to decision regarding disposition that is, admission/referral termed disposition decision (DD) time. Secondary outcomes included length of stay (LOS) at the ambulatory care unit/practice and mortality.
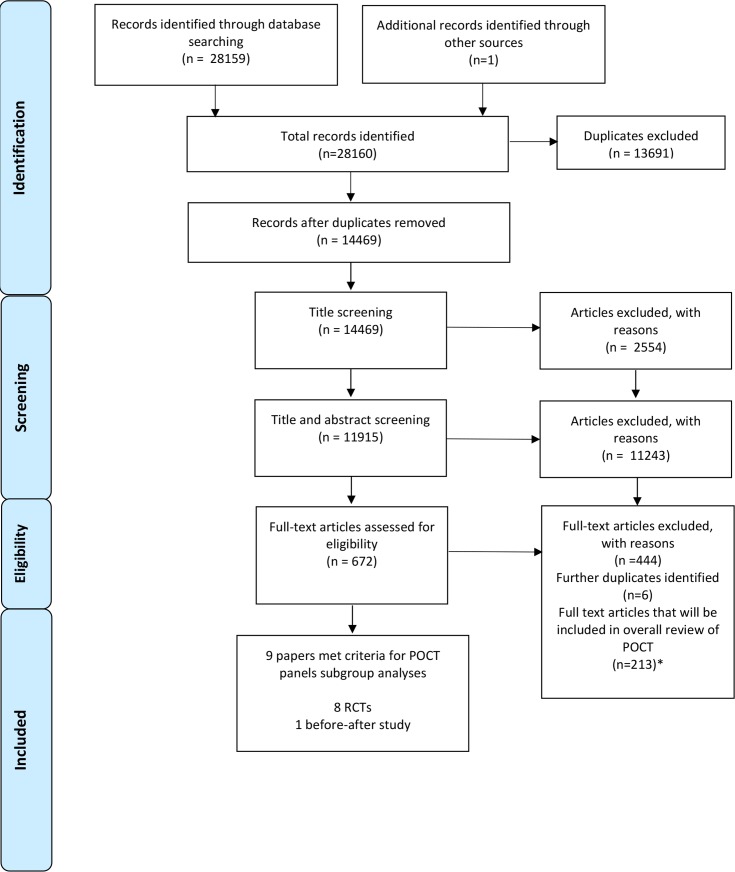
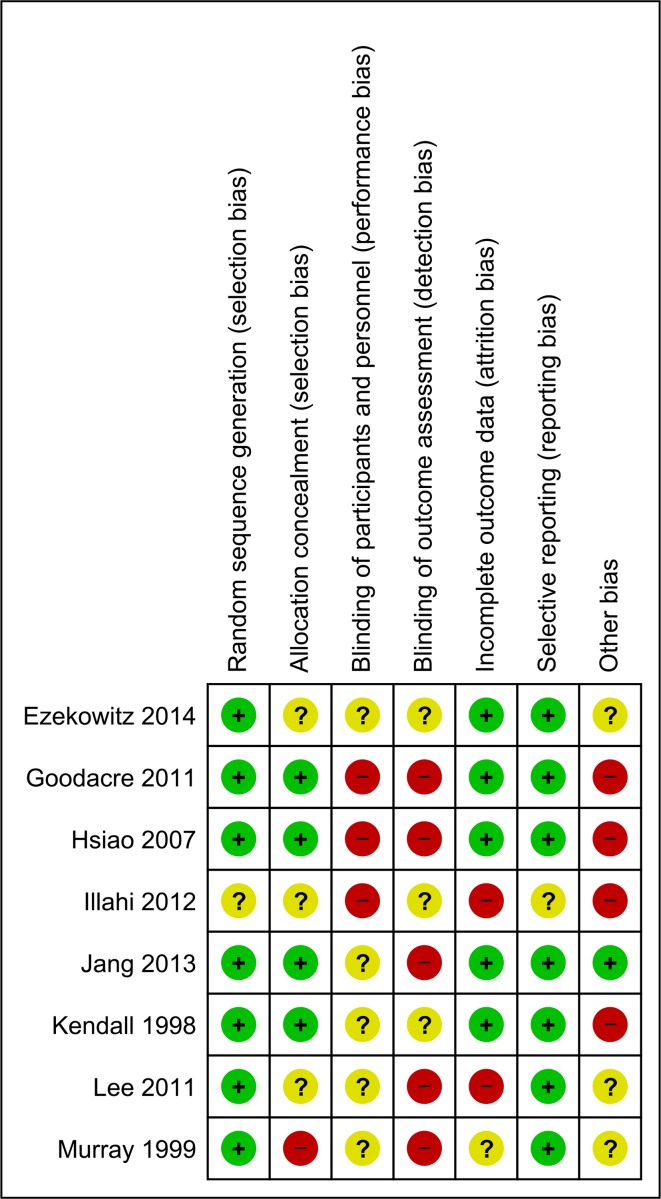
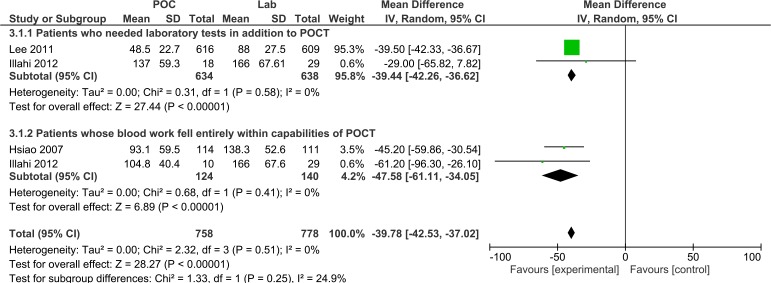
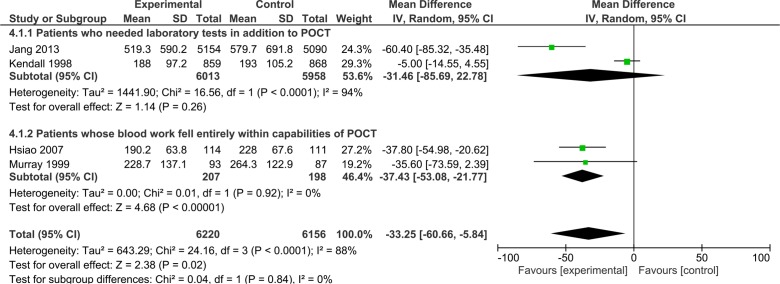
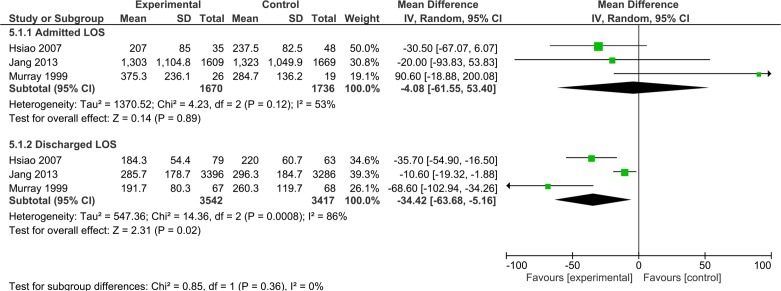
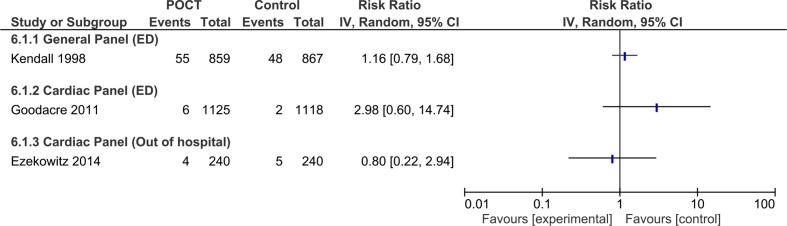
Results: 19 562 patients from nine studies were included in the review, eight of these were randomised-controlled trials, and one was a before-after study. All the studies were based in either emergency departments or the ambulance service; no studies were from primary care settings. General panel tests performed at the POCT resulted in DDs being made 40 min faster (95% CI -42.2 to -36.6, I2=0%) compared with the group receiving usual care, including central laboratory testing. This in turn resulted in a reduction in LOS for patients who were subsequently discharged by 34 min (95% CI -63.7 to -5.16). No significant difference in mortality was reported.
Discussion: Although statistical and clinical heterogeneity is evident and only a small number of studies were included in the meta-analysis, our results suggest that POCTs might lead to faster discharge decisions. Future research should be performed in primary care and identify how POCTs can contribute meaningful changes to patient care rather than focusing on healthcare processes.
Prospero registration number: CRD42016035426.
Keywords: POCT; accident & emergency medicine; chemical pathology; paediatric A&E and ambulatory care; point of care tests; primary care.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources