

T-cell subset abnormalities predict progression along the Inflammatory Arthritis disease continuum: implications for management
- PMID: 32111870
- PMCID: PMC7048829
- DOI: 10.1038/s41598-020-60314-w
T-cell subset abnormalities predict progression along the Inflammatory Arthritis disease continuum: implications for management
Abstract
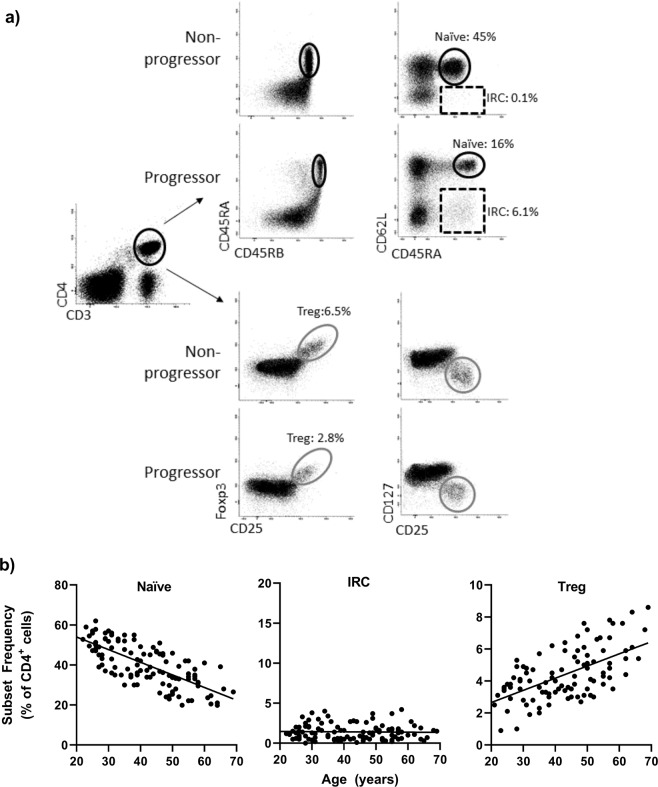
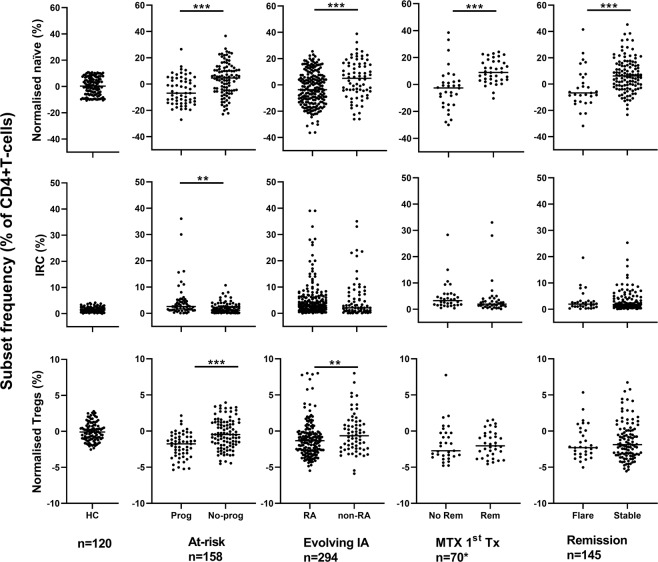
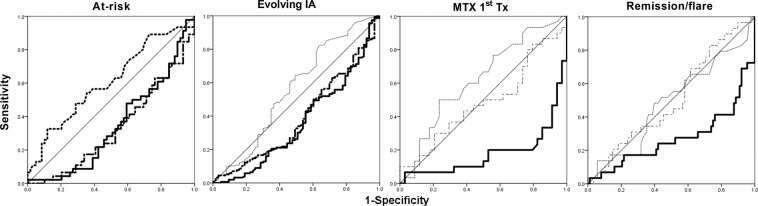
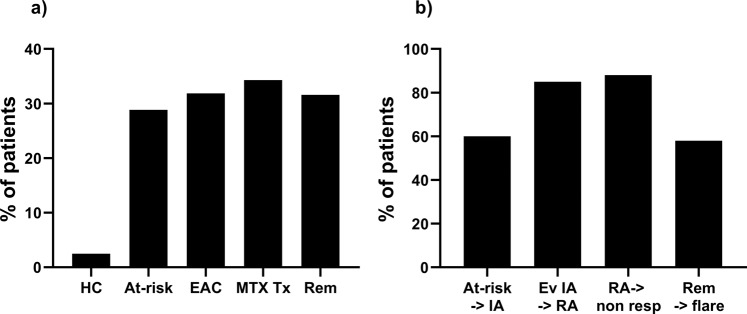
The presence of a disease continuum in inflammatory arthritis (IA) is a recognised concept, with distinct stages from at-risk stage (presence of anti citrullinated-peptide autoantibody) to diagnosis of rheumatoid arthritis (RA), including therapy-induced remission. Despite T-cell dysregulation being a key feature of RA, there are few reports of T-cell phenotyping along the IA-continuum. We investigated the disturbances of naïve, regulatory and inflammation related cell (IRC) CD4+ T-cell subsets in 705 individuals across the IA-continuum, developing a simple risk-score (summing presence/absence of a risk-associated with a subset) to predict progression from one stage to the next. In 158 at-risk individuals, the 3 subsets had individual association with progression to IA and the risk-score was highly predictive (p < 0.0001). In evolving IA patients, 219/294 developed RA; the risk-score included naïve and/or Treg and predicted progression (p < 0.0001). In 120 untreated RA patients, the risk-score for predicting treatment-induced remission using naïve T-cells had an odds ratio of 15.4 (p < 0.0001). In RA patients in treatment-induced remission, a score using naïve T-cells predicted disease flare (p < 0.0001). Evaluating the risk of progression using naïve CD4+ T-cells was predictive of progression along the whole IA-continuum. This should allow identification of individuals at high-risk of progression, permitting targeted therapy for improved outcomes.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Quinn M, Emery P. Window of opportunity in early rheumatoid arthritis: possibility of altering the disease process with early intervention. Clinical and experimental rheumatology. 2003;21:S154–S157. - PubMed
-
- Mankia K, Emery P. Review: Preclinical Rheumatoid Arthritis Progress Toward Prevention. Arthritis &. Rheumatology. 2016;68:779–788. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
