

Review
doi: 10.1245/s10434-020-08221-2.
Epub 2020 Feb 28.
Update on Pheochromocytoma and Paraganglioma from the SSO Endocrine and Head and Neck Disease Site Working Group, Part 2 of 2: Perioperative Management and Outcomes of Pheochromocytoma and Paraganglioma
Affiliations
- PMID: 32112213
- PMCID: PMC8638680
- DOI: 10.1245/s10434-020-08221-2
Item in Clipboard
Review
Update on Pheochromocytoma and Paraganglioma from the SSO Endocrine and Head and Neck Disease Site Working Group, Part 2 of 2: Perioperative Management and Outcomes of Pheochromocytoma and Paraganglioma
Ann Surg Oncol.
2020 May.
Abstract
This is the second part of a two-part review on pheochromocytoma and paragangliomas (PPGLs). In this part, perioperative management, including preoperative preparation, intraoperative, and postoperative interventions are reviewed. Current data on outcomes following resection are presented, including outcomes after cortical-sparing adrenalectomy for bilateral adrenal disease. In addition, pathological features of malignancy, surveillance considerations, and the management of advanced disease are also discussed.
Figures
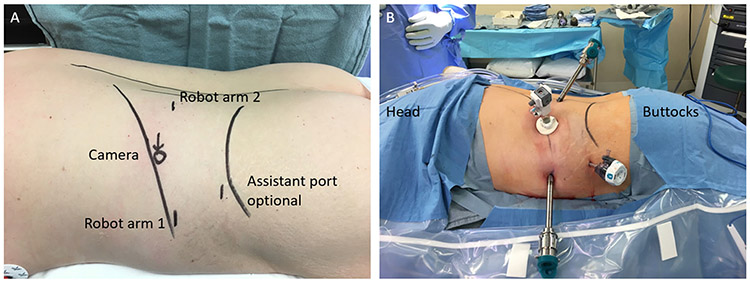
a Diagram outlining port placement for robotic retroperitoneoscopic approach to an adrenalectomy. b Patient prepped, draped, and ports placed for robotic retroperitoneal total adrenalectomy
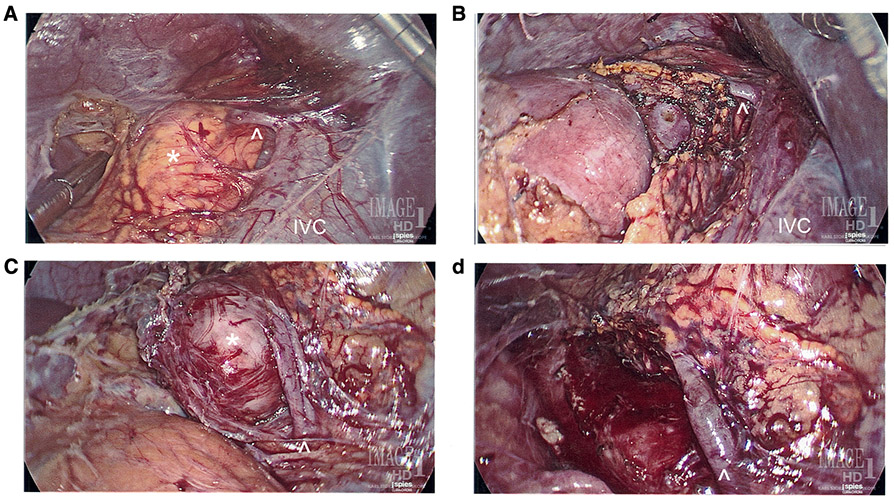
Eleven-year-old male with VHL syndrome who underwent laparoscopic bilateral partial adrenalectomies guided with intraoperative ultrasound for bilateral pheochromocytomas. a Right adrenal tumor measuring 1.8 cm. b Post right partial adrenalectomy with preservation of the right adrenal vein. c Left adrenal tumor measuring 3.0 cm. d Post left partial adrenalectomy with preservation of the left adrenal vein. *Left and right adrenal tumors, respectively, ^Left and right adrenal veins, respectively, IVC inferior vena cava
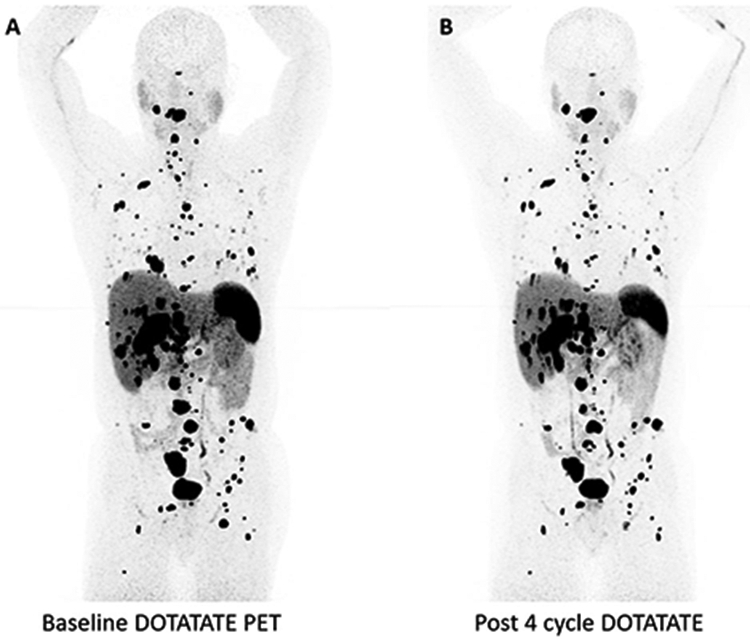
A 59-year-old male with SDHB who underwent PRRT for progressive metastatic PPGL showing mild response after four cycles of treatment. a Baseline 68-gallium DOTATATE PET/CT scan showing widely metastatic disease. b 68-Gallium DOTATATE PET/CT scan showing mild tumor response after four cycles of Lutathera therapy
Similar articles
-
Perioperative outcomes of syndromic paraganglioma and pheochromocytoma resection in patients with von Hippel-Lindau disease, multiple endocrine neoplasia type 2, or neurofibromatosis type 1.Surgery. 2017 Dec;162(6):1259-1269. doi: 10.1016/j.surg.2017.08.002. Epub 2017 Sep 14. Surgery. 2017. PMID: 28919049
-
Update on Pheochromocytoma and Paraganglioma from the SSO Endocrine/Head and Neck Disease-Site Work Group. Part 1 of 2: Advances in Pathogenesis and Diagnosis of Pheochromocytoma and Paraganglioma.Ann Surg Oncol. 2020 May;27(5):1329-1337. doi: 10.1245/s10434-020-08220-3. Epub 2020 Feb 28. Ann Surg Oncol. 2020. PMID: 32112212 Free PMC article. Review.
-
Preoperative Management of Pheochromocytoma and Paraganglioma.Front Endocrinol (Lausanne). 2020 Sep 29;11:586795. doi: 10.3389/fendo.2020.586795. eCollection 2020. Front Endocrinol (Lausanne). 2020. PMID: 33117294 Free PMC article. Review.
-
Surgical management of hereditary pheochromocytoma.J Am Coll Surg. 2004 Apr;198(4):525-34; discussion 534-5. doi: 10.1016/j.jamcollsurg.2003.12.001. J Am Coll Surg. 2004. PMID: 15051000
-
Laparoscopic resection of periadrenal paraganglioma in a patient with multiple endocrine neoplasia type 2A.Surg Laparosc Endosc Percutan Tech. 2011 Feb;21(1):e31-3. doi: 10.1097/SLE.0b013e3182074c72. Surg Laparosc Endosc Percutan Tech. 2011. PMID: 21304370
Cited by
-
Clinical Predictors of Pseudohypoxia-Type Pheochromocytomas.Ann Surg Oncol. 2022 Jun;29(6):3536-3546. doi: 10.1245/s10434-022-11419-1. Epub 2022 Mar 1. Ann Surg Oncol. 2022. PMID: 35233740
-
Pheochromocytoma: Clinical Experience From a Single Tertiary Care Center in India.Cureus. 2023 Jul 10;15(7):e41671. doi: 10.7759/cureus.41671. eCollection 2023 Jul. Cureus. 2023. PMID: 37575861 Free PMC article.
-
Effects of Peptide Receptor Radiotherapy in Patients with Advanced Paraganglioma and Pheochromocytoma: A Nation-Wide Cohort Study.Cancers (Basel). 2024 Mar 29;16(7):1349. doi: 10.3390/cancers16071349. Cancers (Basel). 2024. PMID: 38611027 Free PMC article.
-
Carotid stenosis complicating a vagus paraganglioma: A dually rare case.Int J Surg Case Rep. 2025 Jan;126:110751. doi: 10.1016/j.ijscr.2024.110751. Epub 2024 Dec 17. Int J Surg Case Rep. 2025. PMID: 39706144 Free PMC article.
-
Metastatic Pheochromocytoma and Paraganglioma: Somatostatin Receptor 2 Expression, Genetics, and Therapeutic Responses.J Clin Endocrinol Metab. 2023 Sep 18;108(10):2676-2685. doi: 10.1210/clinem/dgad166. J Clin Endocrinol Metab. 2023. PMID: 36946182 Free PMC article.
References
-
- Kinney MA, Warner ME, van Heerden JA, et al. Perianesthetic risks and outcomes of pheochromocytoma and paraganglioma resection. Anesth Analg. 2000;91(5):1118–1123. - PubMed
-
- Steinsapir J, Carr AA, Prisant LM, Bransome ED Jr. Metyrosine and pheochromocytoma. Arch Intern Med. 1997;157(8):901–906. - PubMed
-
- Wachtel H, Kennedy EH, Zaheer S, et al. Preoperative metyrosine improves cardiovascular outcomes for patients undergoing surgery for pheochromocytoma and paraganglioma. Ann Surg Oncol. 2015;22 Suppl 3:S646–54. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
