

Economic Outcomes in Patients with Chemotherapy-Naïve Metastatic Castration-Resistant Prostate Cancer Treated with Enzalutamide or Abiraterone Acetate Plus Prednisone
- PMID: 32112280
- PMCID: PMC7467473
- DOI: 10.1007/s12325-020-01260-x
Economic Outcomes in Patients with Chemotherapy-Naïve Metastatic Castration-Resistant Prostate Cancer Treated with Enzalutamide or Abiraterone Acetate Plus Prednisone
Abstract
Introduction: Prostate cancer (PC) is the second leading cause of cancer death among US men and accounts for considerable healthcare expenditures. We evaluated economic outcomes in men with chemotherapy-naïve metastatic castration-resistant PC (mCRPC) treated with enzalutamide or abiraterone acetate plus prednisone (abiraterone).
Methods: We performed a retrospective analysis on 3174 men (18 years or older) utilizing the Veterans Health Administration (VHA) database from 1 April 2014 to 31 March 2018. Men with mCRPC were included if they had at least one pharmacy claim for enzalutamide or abiraterone (first claim date = index date) following surgical or medical castration, had no chemotherapy treatment within 12 months prior to the index date, and had continuous VHA enrollment for at least 12 months pre- and post-index date. Men were followed until death, disenrollment, or end of study and were 1:1 propensity score matched (PSM). All-cause and PC-related resource use and costs per patient per month (PPPM) in the 12 months post index were compared between matched cohorts.
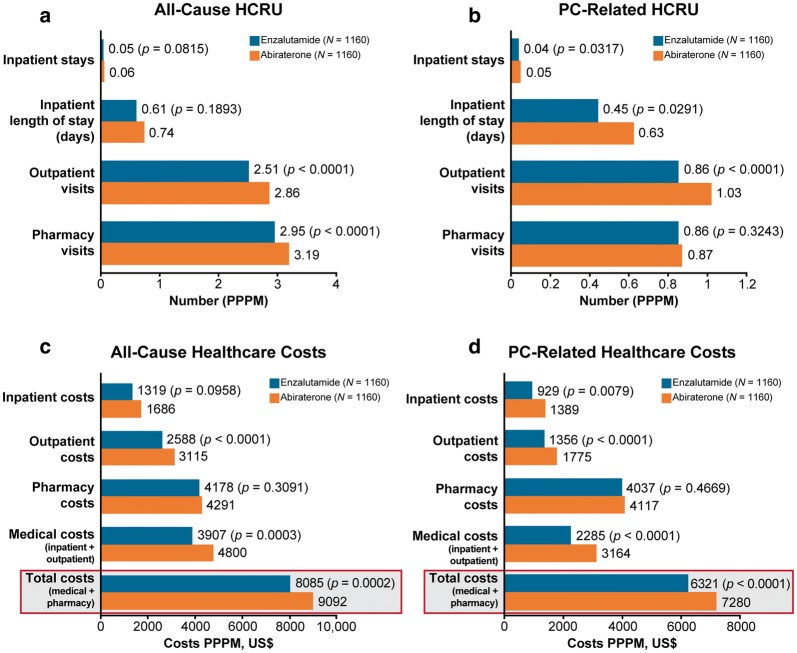
Results: We identified 1229 men with mCRPC prescribed enzalutamide and 1945 prescribed abiraterone with mean ages of 74 and 73 years, respectively. After PSM, each cohort had 1160 patients. The enzalutamide cohort had fewer all-cause (2.51 vs 2.86; p < 0.0001) and PC-related outpatient visits (0.86 vs 1.03; p < 0.0001), with corresponding lower all-cause ($2588 vs $3115; p < 0.0001) and PC-related ($1356 vs $1775; p < 0.0001) PPPM outpatient costs compared with the abiraterone cohort. All-cause total costs (medical and pharmacy) PPPM ($8085 vs $9092; p = 0.0002) and PC-related total costs PPPM ($6321 vs $7280; p < 0.0001) were significantly lower in the enzalutamide cohort compared with the abiraterone cohort.
Conclusions: Enzalutamide-treated men with chemotherapy-naïve mCRPC had significantly lower resource utilization and healthcare costs compared with abiraterone-treated men.
Keywords: Abiraterone acetate; Enzalutamide; Healthcare costs; Prostate cancer; Survival.
Plain language summary
Prostate cancer (PC) is the second leading cause of death among men with cancer in the USA. Healthcare costs associated with PC, including hospitalizations, outpatient visits, and medications prescribed to treat adverse effects, depend on the severity of the disease and intensity of treatment, but are generally very high. Enzalutamide and abiraterone acetate with prednisone (abiraterone) are both approved treatments for men with PC that does not respond to treatments that reduce the male hormone testosterone, known as castration-resistant PC (CRPC). These drugs are associated with varying treatment duration and different adverse effects, and therefore could result in differences in the use of healthcare resources and overall cost of treatment. Here we evaluated the healthcare resource utilization (HCRU), which was calculated as the average number of healthcare encounters, including inpatient stays, outpatient visits, and pharmacy visits, and length of inpatient stays, and treatment costs associated with use of enzalutamide or abiraterone by men with metastatic CRPC (mCRPC), who had not received prior chemotherapy in the Veterans Health Administration. We found that men with chemotherapy-naïve mCRPC treated with enzalutamide used less healthcare resources and incurred lower total healthcare costs than men treated with abiraterone. On average, all-cause total healthcare costs were $1007 per patient per month lower and PC-related total healthcare costs were $959 per patient per month lower for patients treated with enzalutamide than those treated with abiraterone. These results support the hypothesis that the long-term HCRU and costs of enzalutamide may be lower compared with abiraterone.
Figures

Similar articles
-
Treatment Duration, Healthcare Resource Utilization, and Costs Among Chemotherapy-Naïve Patients with Metastatic Castration-Resistant Prostate Cancer Treated with Enzalutamide or Abiraterone Acetate: A Retrospective Claims Analysis.Adv Ther. 2018 Oct;35(10):1639-1655. doi: 10.1007/s12325-018-0774-1. Epub 2018 Sep 6. Adv Ther. 2018. PMID: 30191463 Free PMC article.
-
Cost per median overall survival month associated with abiraterone acetate and enzalutamide for treatment of patients with metastatic castration-resistant prostate cancer.J Med Econ. 2016 Aug;19(8):777-84. doi: 10.3111/13696998.2016.1173042. Epub 2016 Apr 20. J Med Econ. 2016. PMID: 27031255
-
Survival outcomes in patients with chemotherapy-naive metastatic castration-resistant prostate cancer treated with enzalutamide or abiraterone acetate.Prostate Cancer Prostatic Dis. 2021 Dec;24(4):1032-1040. doi: 10.1038/s41391-021-00318-3. Epub 2021 Feb 21. Prostate Cancer Prostatic Dis. 2021. PMID: 33612825 Free PMC article.
-
Matching-adjusted indirect comparison of talazoparib plus enzalutamide versus abiraterone acetate and docetaxel in mCRPC.Future Oncol. 2025 Apr;21(9):1075-1084. doi: 10.1080/14796694.2025.2471200. Epub 2025 Mar 5. Future Oncol. 2025. PMID: 40045559 Free PMC article.
-
Optimal treatment sequencing of abiraterone acetate plus prednisone and enzalutamide in patients with castration-resistant metastatic prostate cancer: A systematic review and meta-analysis.Cancer Treat Rev. 2021 Feb;93:102152. doi: 10.1016/j.ctrv.2020.102152. Epub 2021 Jan 11. Cancer Treat Rev. 2021. PMID: 33486302
Cited by
-
Outcomes Following Abiraterone versus Enzalutamide for Prostate Cancer: A Scoping Review.Cancers (Basel). 2022 Aug 3;14(15):3773. doi: 10.3390/cancers14153773. Cancers (Basel). 2022. PMID: 35954437 Free PMC article.
-
Treatment patterns and outcomes in patients with nonmetastatic castration-resistant prostate cancer in the United States.Future Oncol. 2024;20(32):2467-2480. doi: 10.1080/14796694.2024.2373681. Epub 2024 Jul 29. Future Oncol. 2024. PMID: 39073610 Free PMC article.
-
Healthcare Costs in Men with Metastatic Castration-Resistant Prostate Cancer: An Analysis of US Medicare Fee-For-Service Claims.Adv Ther. 2023 Oct;40(10):4480-4492. doi: 10.1007/s12325-023-02572-4. Epub 2023 Aug 2. Adv Ther. 2023. PMID: 37531024 Free PMC article.
-
Salvage Ultrasound-Guided Robot-Assisted Video-Endoscopic Inguinal Lymphadenectomy (RAVEIL) as a Metastasis-Directed Therapy (MDT) in Oligoprogressive Metastatic Castration-Resistant Prostate Cancer (mCRPC): A Case Report and Review of the Literature.Curr Oncol. 2025 Feb 18;32(2):115. doi: 10.3390/curroncol32020115. Curr Oncol. 2025. PMID: 39996915 Free PMC article. Review.
-
Cost-effectiveness and budget impact analysis of enzalutamide in comparison to abiraterone in treatment of metastatic prostate cancer resistant to castration in Iran.BMC Urol. 2024 Feb 20;24(1):45. doi: 10.1186/s12894-024-01431-w. BMC Urol. 2024. PMID: 38378521 Free PMC article.
References
-
- SEER. SEER Explorer. Surveillance, Epidemiology, and End Results Program; National Cancer Institute. 2019. https://seer.cancer.gov/explorer/application.php?site=66&data_type=4&gra.... Accessed Nov 14, 2019.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
