

Cardiovascular magnetic resonance in immune checkpoint inhibitor-associated myocarditis
- PMID: 32112560
- PMCID: PMC7205467
- DOI: 10.1093/eurheartj/ehaa051
Cardiovascular magnetic resonance in immune checkpoint inhibitor-associated myocarditis
Abstract
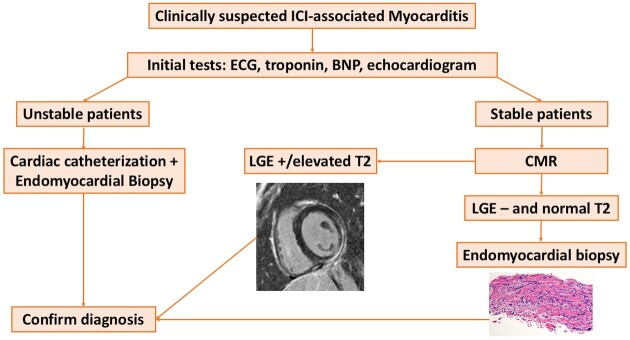
Aims: Myocarditis is a potentially fatal complication of immune checkpoint inhibitors (ICI). Sparse data exist on the use of cardiovascular magnetic resonance (CMR) in ICI-associated myocarditis. In this study, the CMR characteristics and the association between CMR features and cardiovascular events among patients with ICI-associated myocarditis are presented.
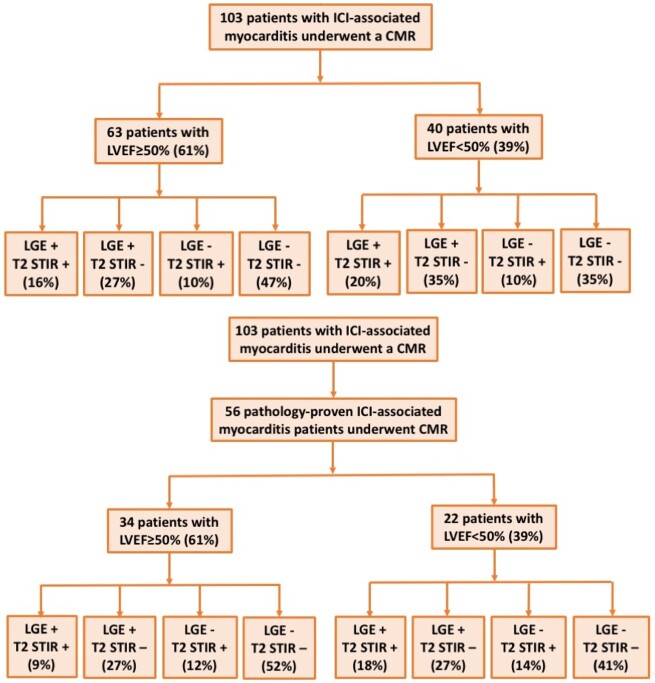
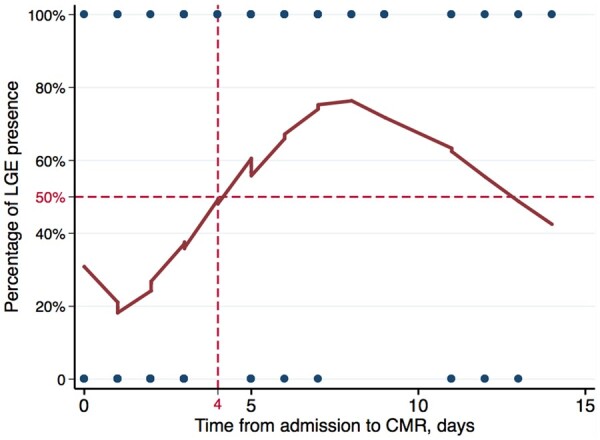
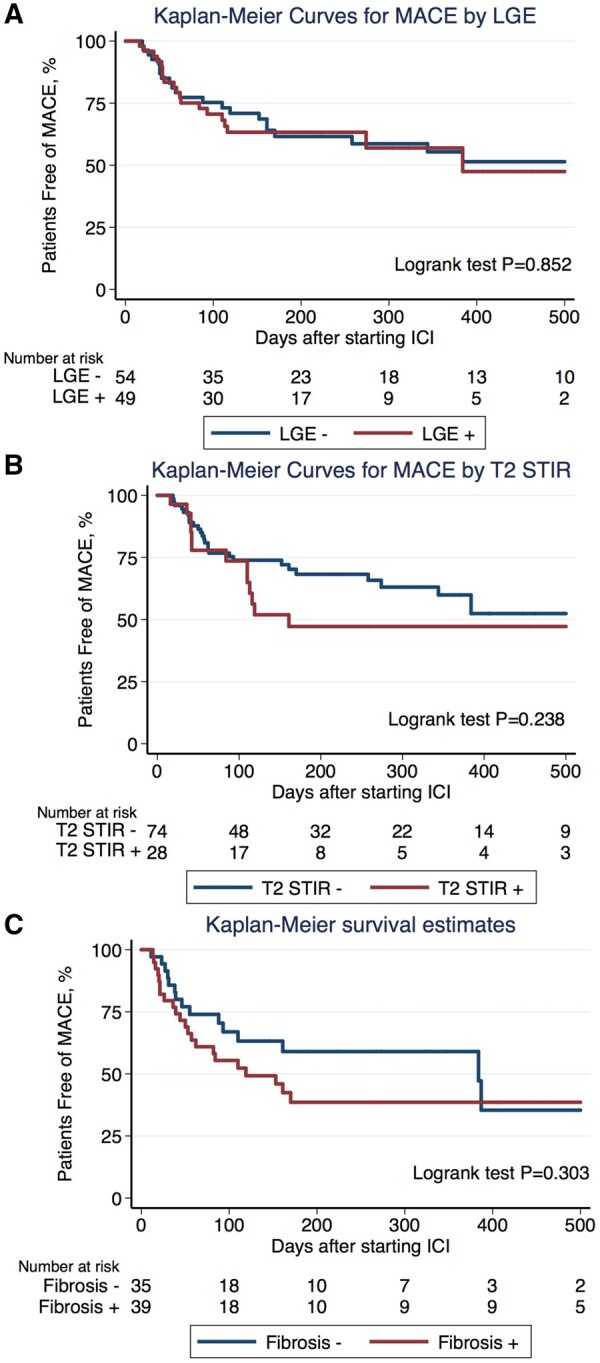
Methods and results: From an international registry of patients with ICI-associated myocarditis, clinical, CMR, and histopathological findings were collected. Major adverse cardiovascular events (MACE) were a composite of cardiovascular death, cardiogenic shock, cardiac arrest, and complete heart block. In 103 patients diagnosed with ICI-associated myocarditis who had a CMR, the mean left ventricular ejection fraction (LVEF) was 50%, and 61% of patients had an LVEF ≥50%. Late gadolinium enhancement (LGE) was present in 48% overall, 55% of the reduced EF, and 43% of the preserved EF cohort. Elevated T2-weighted short tau inversion recovery (STIR) was present in 28% overall, 30% of the reduced EF, and 26% of the preserved EF cohort. The presence of LGE increased from 21.6%, when CMR was performed within 4 days of admission to 72.0% when CMR was performed on Day 4 of admission or later. Fifty-six patients had cardiac pathology. Late gadolinium enhancement was present in 35% of patients with pathological fibrosis and elevated T2-weighted STIR signal was present in 26% with a lymphocytic infiltration. Forty-one patients (40%) had MACE over a follow-up time of 5 months. The presence of LGE, LGE pattern, or elevated T2-weighted STIR were not associated with MACE.
Conclusion: These data suggest caution in reliance on LGE or a qualitative T2-STIR-only approach for the exclusion of ICI-associated myocarditis.
Keywords: Cardiovascular magnetic resonance; Immune checkpoint inhibitor; Myocarditis.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2020. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Immune checkpoint inhibitor cardiotoxicity: what can we learn from real life data on CMR as a diagnostic tool?Eur Heart J. 2020 May 7;41(18):1744-1746. doi: 10.1093/eurheartj/ehaa136. Eur Heart J. 2020. PMID: 32176277 No abstract available.
References
-
- Hodi FS, O'Day SJ, McDermott DF, Weber RW, Sosman JA, Haanen JB, Gonzalez R, Robert C, Schadendorf D, Hassel JC, Akerley W, van den Eertwegh AJM, Lutzky J, Lorigan P, Vaubel JM, Linette GP, Hogg D, Ottensmeier CH, Lebbé C, Peschel C, Quirt I, Clark JI, Wolchok JD, Weber JS, Tian J, Yellin MJ, Nichol GM, Hoos A, Urba WJ. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med 2010;363:711–723. - PMC - PubMed
-
- Robert C, Thomas L, Bondarenko I, O'Day S, Weber J, Garbe C, Lebbe C, Baurain J-F, Testori A, Grob J-J, Davidson N, Richards J, Maio M, Hauschild A, Miller WH, Gascon P, Lotem M, Harmankaya K, Ibrahim R, Francis S, Chen T-T, Humphrey R, Hoos A, Wolchok JD. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N Engl J Med 2011;364:2517–2526. - PubMed
-
- Postow MA, Sidlow R, Hellmann MD. Immune-related adverse events associated with immune checkpoint blockade. N Engl J Med 2018;378:158–168. - PubMed
-
- Tang J, Shalabi A, Hubbard-Lucey VM. Comprehensive analysis of the clinical immuno-oncology landscape. Ann Oncol 2018;29:84–91. - PubMed
-
- Nghiem PT, Bhatia S, Lipson EJ, Kudchadkar RR, Miller NJ, Annamalai L, Berry S, Chartash EK, Daud A, Fling SP, Friedlander PA, Kluger HM, Kohrt HE, Lundgren L, Margolin K, Mitchell A, Olencki T, Pardoll DM, Reddy SA, Shantha EM, Sharfman WH, Sharon E, Shemanski LR, Shinohara MM, Sunshine JC, Taube JM, Thompson JA, Townson SM, Yearley JH, Topalian SL, Cheever MA. PD-1 blockade with pembrolizumab in advanced merkel-cell carcinoma. N Engl J Med 2016;374:2542–2552. - PMC - PubMed
