

Diagnostic and prognostic value of T-wave amplitude difference between supine and orthostatic electrocardiogram in children and adolescents with postural orthostatic tachycardia syndrome
- PMID: 32112609
- PMCID: PMC7358833
- DOI: 10.1111/anec.12747
Diagnostic and prognostic value of T-wave amplitude difference between supine and orthostatic electrocardiogram in children and adolescents with postural orthostatic tachycardia syndrome
Abstract
Objective: To investigate the diagnostic and prognostic value of T-wave amplitude difference between supine and orthostatic electrocardiogram (ECG) in children and adolescents with postural orthostatic tachycardia syndrome (POTS).
Methods: A total of 100 children and adolescents (POTS group, 50 males and 50 females, aged at 11.0 ± 2.4 years) diagnosed as POTS were enrolled from August 2013 to July 2016. Seventy-one children were matched as the control group according to age and sex. All cases completed the supine and orthostatic ECG.
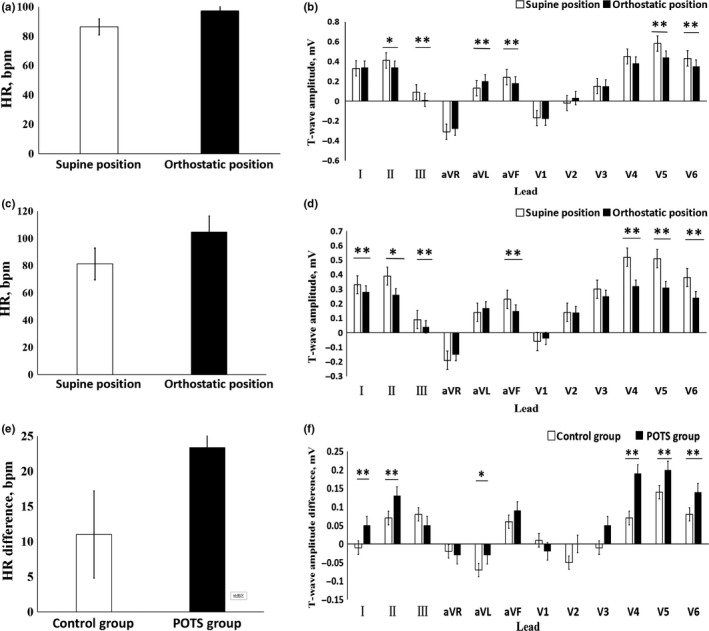
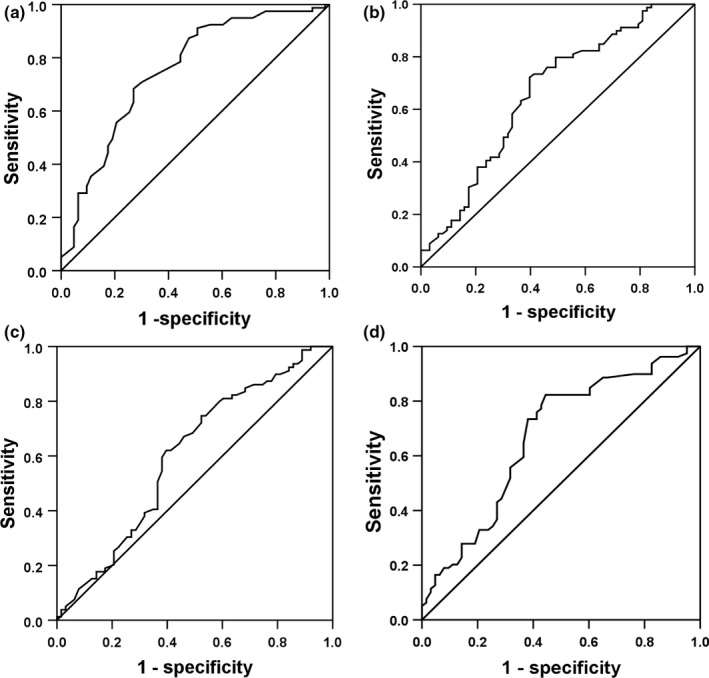
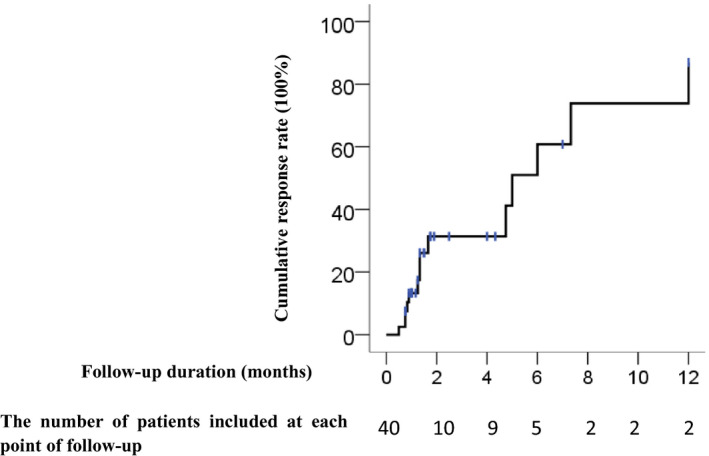
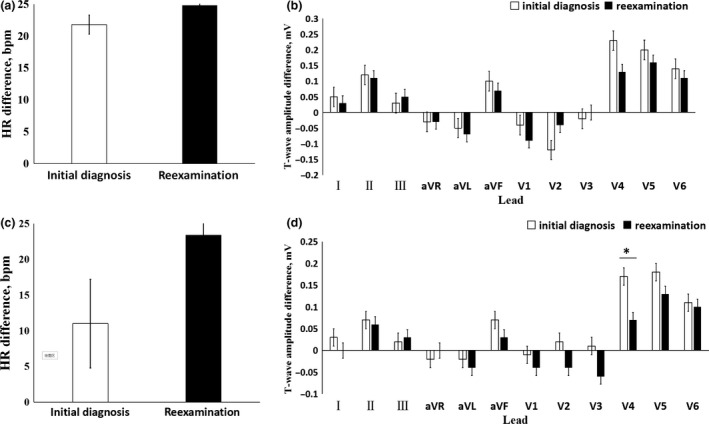
Results: (a) Compared with the control group, the T-wave amplitude difference in leads I, II, aVL, V4 , V5, and V6 and the heart rate (HR) difference increased in POTS group. (b) Logistic regression analysis: The T-wave amplitude difference in leads V4 , V5 , and V6 and HR difference have statistical significance for POTS diagnosis. (c) Diagnostic test evaluation: When HR difference was ≥ 15 times/min, T-wave amplitude difference in lead V5 was ≥0.15 mV, T-wave amplitude difference in leads V4 and V6 were ≥0.10 mV, and the sensitivity and specificity of POTS diagnosis were 35.0% and 88.7%. (d) Follow-up: There was no significant difference in HR difference and T-wave amplitude difference in the nonresponse groups. In the response group, the T-wave amplitude difference in lead V4 was reduced than the initial value.
Conclusions: The HR difference and T-wave amplitude difference in leads V4, V5, and V6 between supine and orthostatic ECG are of help in assisting the diagnosis of POTS but no obviously significance on prognosis estimation of it.
Keywords: adolescents; children; electrocardiography; orthostatic position; postural orthostatic tachycardia syndrome; supine position.
© 2020 The Authors. Annals of Noninvasive Electrocardiology published by Wiley Periodicals, Inc.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
-
- Baumert, M. , Lambert, E. , Vaddadi, G. , Sari, C. I. , Esler, M. , Lambert, G. , … Nalivaiko, E. (2011). Cardiac repolarization variability in patients with postural tachycardia syndrome during graded head‐up tilt. Clinical Neurophysiology, 122(2), 405–409. 10.1016/j.clinph.2010.06.017 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
