

Enlarged cardiophrenic lymph nodes predict disease involvement of the upper abdomen and the outcome of primary surgical debulking in advanced ovarian cancer
- PMID: 32112653
- PMCID: PMC7496971
- DOI: 10.1111/aogs.13835
Enlarged cardiophrenic lymph nodes predict disease involvement of the upper abdomen and the outcome of primary surgical debulking in advanced ovarian cancer
Abstract
Introduction: The outcome of ovarian cancer patients is highly dependent on the success of primary debulking surgery in terms of postoperative residual disease. This study critically evaluates the clinical impact of preoperative radiologic assessment of the cardiophrenic lymph node (CPLN) status in advanced ovarian cancer.
Material and methods: Baseline CT scans of 178 stage III and IV ovarian cancer patients were retrospectively reviewed by two independent radiologists. CPLN enlargement defined at a short-axis ≥5 mm was evaluated for its prognostic value and predictive power of upper abdominal tumor involvement and the chance of complete intra-abdominal tumor resection at primary debulking surgery. Only patients without surgically removed CPLN were eligible for this study.
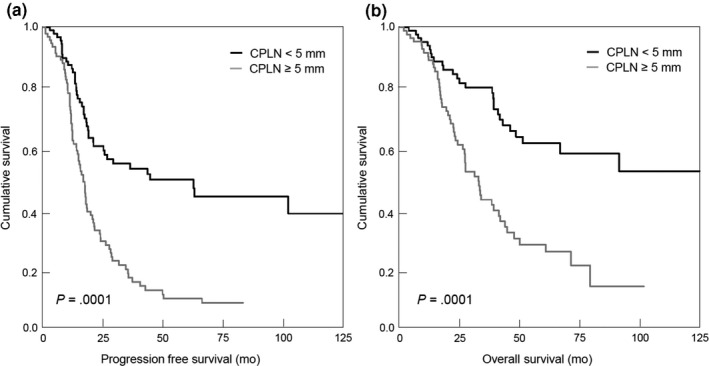
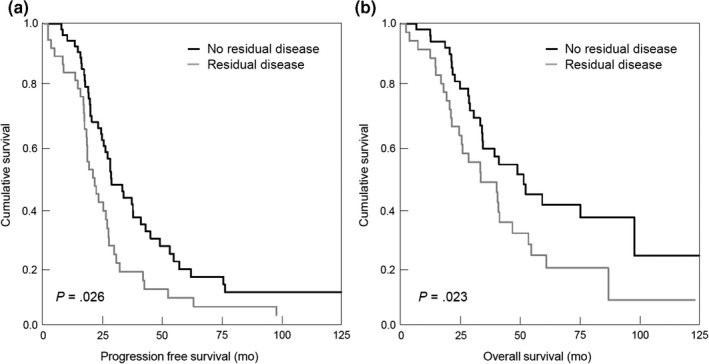
Results: Enlarged CPLNs were detected in 50% of patients and correlated with radiologically suspicious (P = .028) and histologically confirmed (P = .001) paraaortic lymph node metastases. CPLNs ≥ 5 mm were associated with high CA-125 levels at baseline and revealed independent prognostic relevance for progression-free survival (hazard ratio [HR] 2.14, 95% confidence interval [CI] 1.33-3.42) and overall survival (HR 2.18, 95% CI 1.16-4.08). Noteworthy, patients with enlarged CPLNs nonetheless benefit from complete intra-abdominal tumor debulking in terms of an improvement in progression-free survival (HR 0.60, 95% CI 0.38-0.94) and overall survival (HR 0.59, 95% CI 0.35-0.82). Enlarged CPLNs correctly predicted carcinomatosis of the upper abdomen in 94.6%. A predictive score of complete tumor debulking, termed CD-score, which integrates, beside a CPLN short axis <5 mm, an ascites volume <500 mL, and CA-125 levels <500 U/mL at baseline, correctly predicted complete intra-abdominal debulking in 100% of patients.
Conclusions: CPLNs ≥5 mm predict upper abdominal tumor involvement. The application of the CD-score predicted complete macroscopic tumor resection at primary surgery in all of the patients. Although, CPLN pathology suggests extra-abdominal disease, we consistently demonstrated that patients nonetheless benefit from complete intra-abdominal tumor resection.
Keywords: cardiophrenic lymph node; ovarian cancer; predictive value; prognostic impact; residual disease.
2020 The Authors. Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic.
Conflict of interest statement
The authors have stated explicitly that there is no conflict of interest in connection with this article.
Figures
References
-
- Shaaban A, Rezvani M. Ovarian cancer: detection and radiologic staging. Clin Obstet Gynecol. 2009;52:73‐93. - PubMed
-
- du Bois A, Reuss A, Pujade‐Lauraine E, Harter P, Ray‐Coquard I, Pfisterer J. Role of surgical outcome as prognostic factor in advanced epithelial ovarian cancer: a combined exploratory analysis of 3 prospectively randomized phase 3 multicenter trials: by the Arbeitsgemeinschaft Gynaekologische Onkologie Studiengruppe Ovarialkarzinom (AGO‐OVAR) and the Groupe d'Investigateurs Nationaux Pour les Etudes des Cancers de l'Ovaire (GINECO). Cancer. 2009;115:1234‐1244. - PubMed
-
- Harter P, Sehouli J, Lorusso D, et al. A randomized trial of lymphadenectomy in patients with advanced ovarian neoplasms. N Engl J Med. 2019;380:822‐832. - PubMed
-
- LaFargue CJ, Bristow RE. Transdiaphragmatic cardiophrenic lymph node resection for Stage IV ovarian cancer. Gynecol Oncol. 2015;138:762‐763. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
