

Positive follow-up blood cultures identify high mortality risk among patients with Gram-negative bacteraemia
- PMID: 32114010
- PMCID: PMC7311251
- DOI: 10.1016/j.cmi.2020.01.025
Positive follow-up blood cultures identify high mortality risk among patients with Gram-negative bacteraemia
Abstract
Objectives: The role of follow-up blood cultures (FUBCs) in the management of Gram-negative bacteraemia (GNB) is poorly understood. We aimed to determine the utility of FUBCs in identifying patients with increased mortality risk.
Methods: An observational study with a prospectively enrolled cohort of adult inpatients with GNB was conducted at Duke University Health System from 2002 to 2015. FUBCs were defined as blood cultures performed from 24 hours to 7 days from initial positive blood culture.
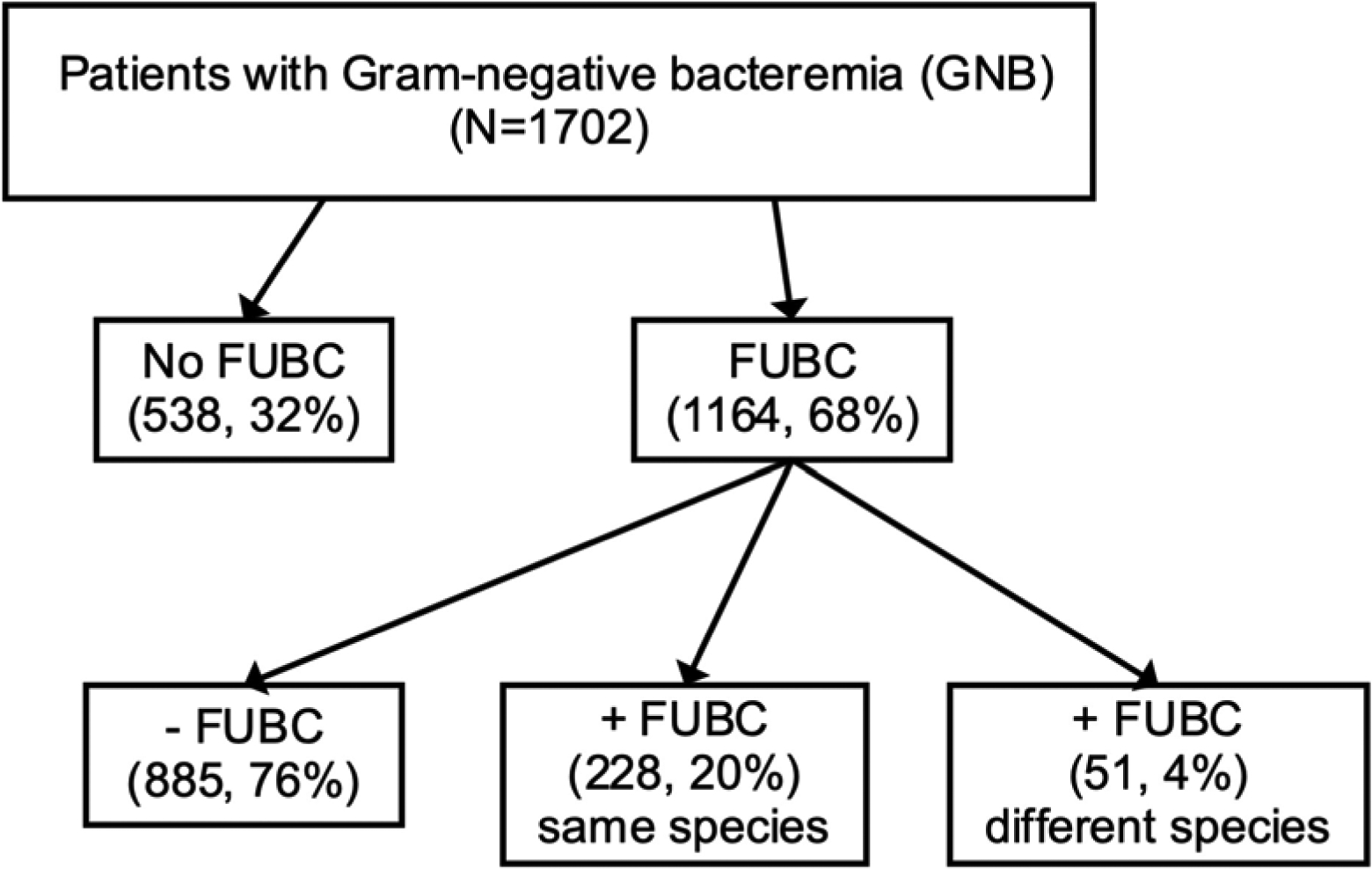
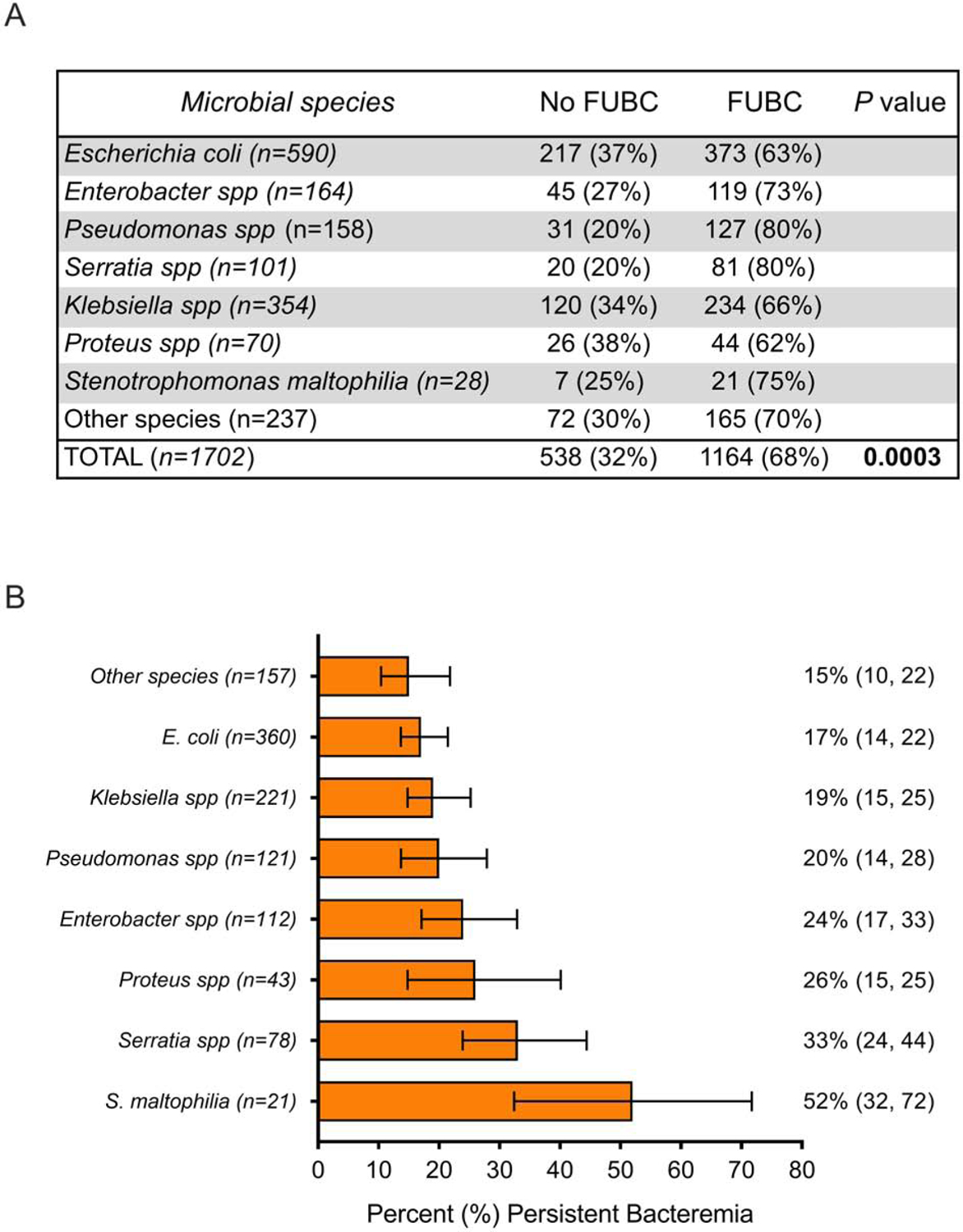
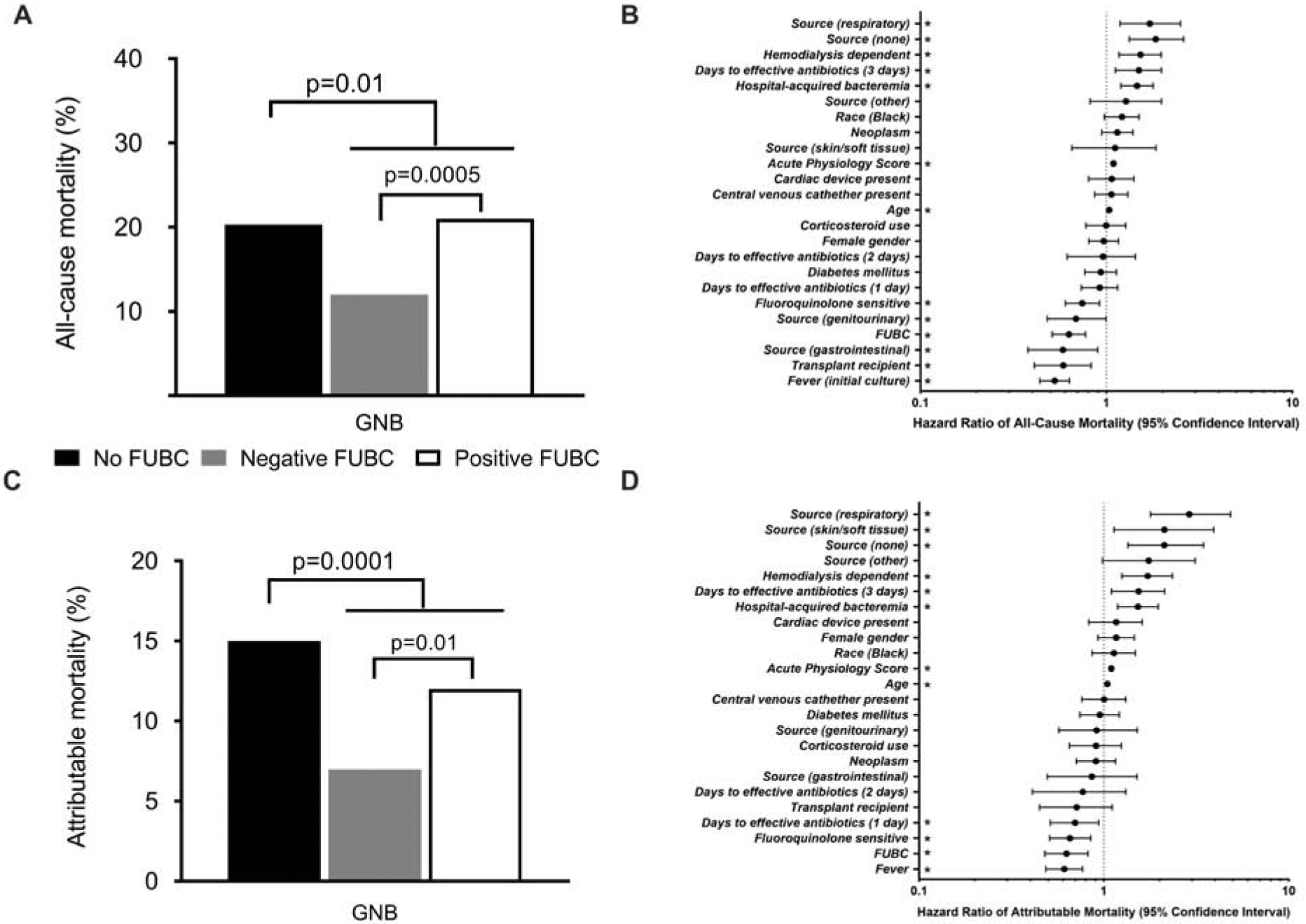
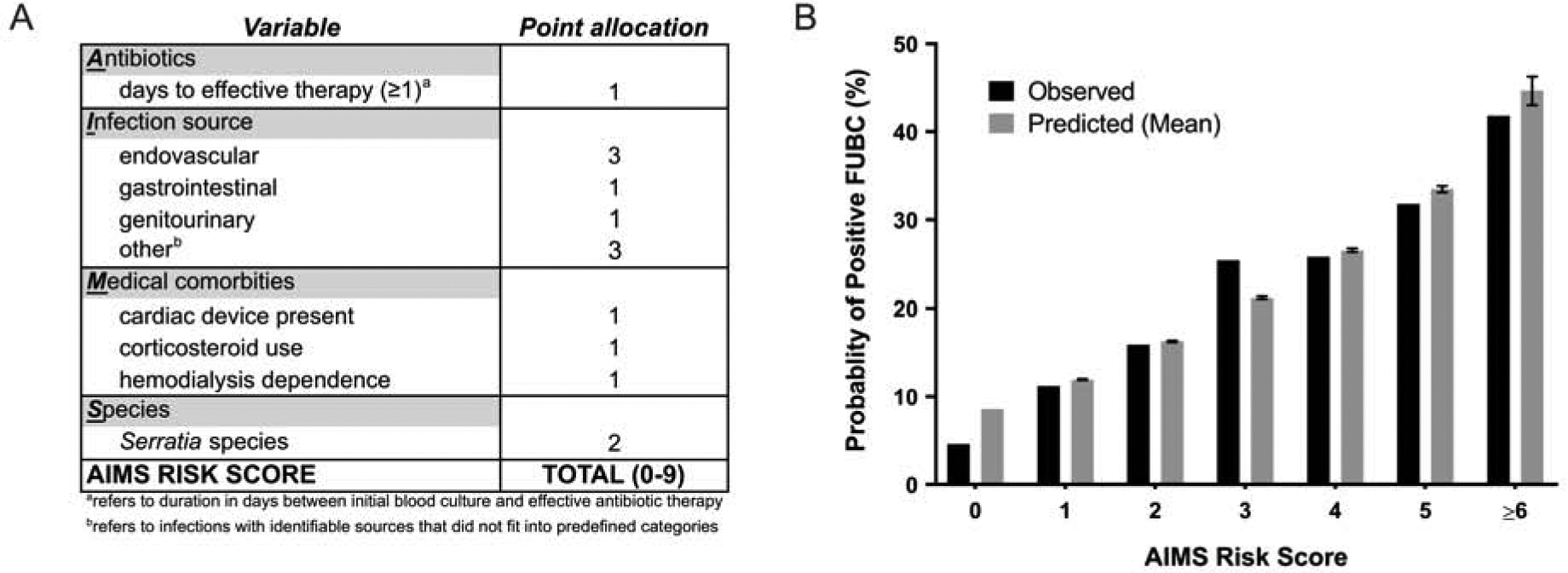
Results: Among 1702 patients with GNB, 1164 (68%) had FUBCs performed. When performed, FUBCs were positive in 20% (228/1113) of cases. FUBC acquisition was associated with lower all-cause in-hospital mortality (108/538, 20%, vs. 176/1164, 15%; p 0.01) and attributable in-hospital mortality (78/538, 15%, vs. 98/1164, 8%; p < 0.0001). Propensity score-weighted Cox proportional hazards models revealed that obtaining FUBCs was associated with reductions in all-cause (hazard ratio (HR) 0.629; 95% confidence interval (CI), 0.511-0.772; p < 0.0001) and attributable mortality (HR 0.628; 95% CI, 0.480-0.820; p 0.0007). Positive FUBCs were associated with increased all-cause mortality (49/228, 21%, vs. 110/885, 11%; p 0.0005) and attributable mortality (27/228, 12%, vs. 61/885, 7%; p 0.01) relative to negative FUBCs. Propensity score-weighted Cox proportional hazards models revealed that positive FUBCs were associated with increased all-cause (HR 2.099; 95% CI, 1.567-2.811; p < 0.0001) and attributable mortality (HR 1.800; 95% CI, 1.245-2.603; p 0.002). In a calibration analysis, a scoring system accurately identified patients at high risk of positive FUBCs.
Conclusions: Rates of positive FUBCs were high and identified patients at increased risk for mortality. Clinical variables can identify patients at high risk for positive FUBCs. FUBCs should be considered in the management of GNB.
Keywords: Blood cultures; Gram-negative bacteremia; Persistent bacteremia; Risk score.
Copyright © 2020 European Society of Clinical Microbiology and Infectious Diseases. Published by Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflict of interest
V.G.F served as Chair of V710 Scientific Advisory Committee (Merck); has received grant support from Cerexa/Actavis/Allergan, Pfizer, Advanced Liquid Logics, NIH, MedImmune, Basilea, Karius, Contrafect, Regeneron, and Genentech; has NIH STTR/SBIR grants pending with Affinergy, Locus, and Medical Surface, Inc; has been a paid consultant for Achaogen, Astellas, Arsanis, Affinergy, Basilea, Bayer, Cerexa, Contrafect, Cubist, Debiopharm, Durata, Grifols, Genentech, MedImmune, Merck, Medicines Co., Pfizer, Novartis, Novadigm, Theravance, xBiotech, and has received honoraria from Theravance, Green Cross, and has a patent pending in sepsis diagnostics. D.v.D. has been a paid consultant for Allergan, Achaogen, Shionogi, Tetraphase, Sanofi-Pasteur, T2 Biosystems, NeuMedicine, Roche, MedImmune, Astellas, and Merck, and received grant support from NIH, Steris, and Scynexis. Travel reimbursement from IDSA, ASM and ESCMID. T.L. is on the scientific board for Motif; has been a paid consultant for Allergan, Paratek, Melinta, Nabriva, Merck, and Motif; has received grants from Motif and Merck; and has received payment for lectures for Motif and Sunovion. Other authors have no competing interests.
Figures
References
-
- Kang CI, Song JH, Chung DR, Peck KR, Ko KS, Yeom JS, et al. Risk factors and pathogenic significance of severe sepsis and septic shock in 2286 patients with gram-negative bacteremia. J Infect 2011;62(1):26–33. - PubMed
-
- Rannikko J, Syrjanen J, Seiskari T, Aittoniemi J, Huttunen R. Sepsis-related mortality in 497 cases with blood culture-positive sepsis in an emergency department. Int J Infect Dis. 2017;58:52–7. - PubMed
-
- Canzoneri CN, Akhavan BJ, Tosur Z, Andrade PEA, Aisenberg GM. Follow-up Blood Cultures in Gram-Negative Bacteremia: Are They Needed? Clin Infect Dis. 2017;65(11):1776–9. - PubMed
