

Decreasing Delirium Through Music: A Randomized Pilot Trial
- PMID: 32114612
- PMCID: PMC7666845
- DOI: 10.4037/ajcc2020175
Decreasing Delirium Through Music: A Randomized Pilot Trial
Abstract
Background: Management of delirium in intensive care units is challenging because effective therapies are lacking. Music is a promising nonpharmacological intervention.
Objectives: To determine the feasibility and acceptability of personalized music (PM), slow-tempo music (STM), and attention control (AC) in patients receiving mechanical ventilation in an intensive care unit, and to estimate the effect of music on delirium.
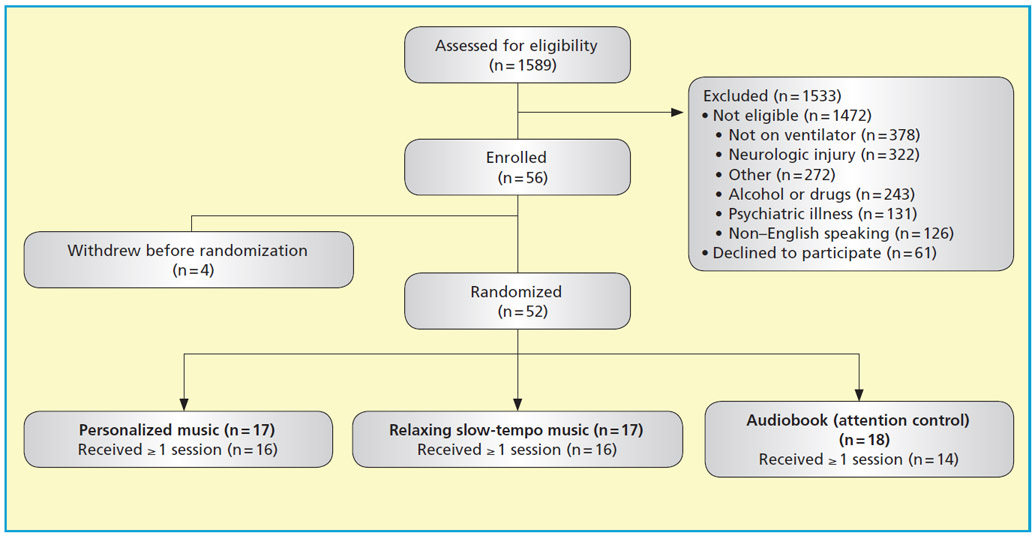
Methods: A randomized controlled trial was performed in an academic medical-surgical intensive care unit. After particular inclusion and exclusion criteria were applied, patients were randomized to groups listening to PM, relaxing STM, or an audiobook (AC group). Sessions lasted 1 hour and were given twice daily for up to 7 days. Patients wore noise-canceling headphones and used mp3 players to listen to their music/audiobook. Delirium and delirium severity were assessed twice daily by using the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) and the CAM-ICU-7, respectively.
Results: Of the 1589 patients screened, 117 (7.4%) were eligible. Of those, 52 (44.4%) were randomized, with a recruitment rate of 5 patients per month. Adherence was higher in the groups listening to music (80% in the PM and STM groups vs 30% in the AC group; P = .01), and 80% of patients surveyed rated the music as enjoyable. The median number (interquartile range) of delirium/coma-free days by day 7 was 2 (1-6) for PM, 3 (1-6) for STM, and 2 (0-3) for AC (P = .32). Median delirium severity was 5.5 (1-7) for PM, 3.5 (0-7) for STM, and 4 (1-6.5) for AC (P = .78).
Conclusions: Music delivery is acceptable to patients and is feasible in intensive care units. Further research testing use of this promising intervention to reduce delirium is warranted.
©2020 American Association of Critical-Care Nurses.
References
-
- Ely EW, Inouye SK, Bernard GR, et al. Delirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU). JAMA. 2001;286(21):2703–2710. - PubMed
-
- Ely EW, Margolin R, Francis J, et al. Evaluation of delirium in critically ill patients: validation of the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU). Crit Care Med. 2001;29(7):1370–1379. - PubMed
-
- Ely EW, Shintani A, Truman B, et al. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. 2004;291(14):1753–1762. - PubMed
-
- McNicoll L, Pisani MA, Zhang Y, Ely EW, Siegel MD, Inouye SK. Delirium in the intensive care unit: occurrence and clinical course in older patients. J Am Geriatr Soc. 2003;51(5):591–598. - PubMed
-
- Miller RR 3rd, Ely EW. Delirium and cognitive dysfunction in the intensive care unit. Semin Respir Crit Care Med. 2006; 27(3):210–220. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 HL130881/HL/NHLBI NIH HHS/United States
- U24 CA092656/CA/NCI NIH HHS/United States
- R01 AG040220/AG/NIA NIH HHS/United States
- R01 NR009295/NR/NINR NIH HHS/United States
- UL1 TR001108/TR/NCATS NIH HHS/United States
- R01 AG055391/AG/NIA NIH HHS/United States
- K23 AG043476/AG/NIA NIH HHS/United States
- R01 AG034205/AG/NIA NIH HHS/United States
- R01 HL131730/HL/NHLBI NIH HHS/United States
- TL1 TR001107/TR/NCATS NIH HHS/United States
- P30 HS024384/HS/AHRQ HHS/United States
- R01 AG030618/AG/NIA NIH HHS/United States
- R24 CA092656/CA/NCI NIH HHS/United States
- P30 AG010133/AG/NIA NIH HHS/United States
