

Clinical Results of Surgical Resection and Histopathological Evaluation of Synovial Chondromatosis in the Shoulder: A Retrospective Study and Literature Review
- PMID: 32117541
- PMCID: PMC7031439
- DOI: 10.4055/cios.2020.12.1.68
Clinical Results of Surgical Resection and Histopathological Evaluation of Synovial Chondromatosis in the Shoulder: A Retrospective Study and Literature Review
Abstract
Background: Synovial chondromatosis occurs rarely in the shoulder, and its details remain unclear. The purpose of this study was to clarify the clinical results of surgical resection and the histopathological findings of synovial chondromatosis in the shoulder.
Methods: Ten shoulders with synovial chondromatosis that had been operatively resected were reviewed retrospectively. Osteochondral lesions were present in the glenohumeral joint in six shoulders and in the subacromial space in four shoulders. Two patients had a history of trauma with glenohumeral dislocation without recurrent instability, and the other seven patients (eight shoulders) did not have any traumatic episodes or past illness involving the ipsilateral shoulder girdle. The occurrences of osteochondral lesions, inferior humeral osteophytes, and acromial spurs were assessed on radiographs before resection, just after resection, and at final follow-up. The Constant scores were compared before resection and at final follow-up with Wilcoxon signed-rank tests. Resected lesions were histopathologically differentiated between primary and secondary synovial chondromatosis.
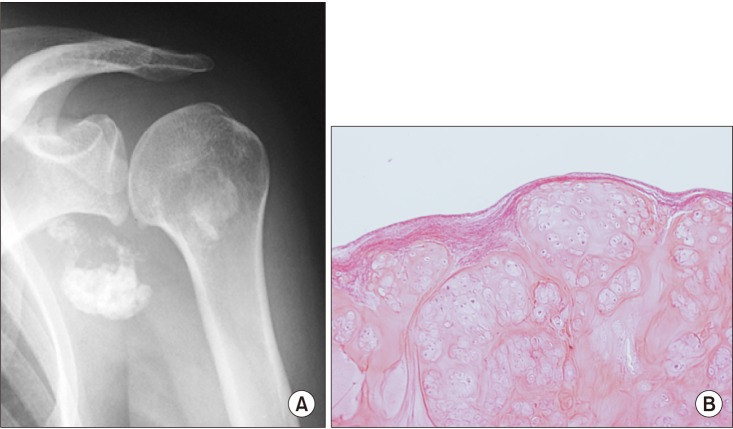
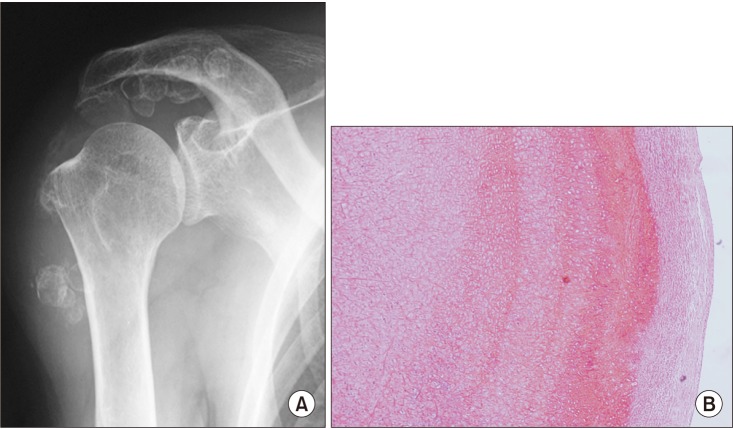
Results: Inferior humeral osteophytes were found in five shoulders with synovial chondromatosis in the glenohumeral joint, and all four shoulders with synovial chondromatosis in the subacromial space had acromial spur formation. Osteochondral lesions appeared to have been successfully removed in all shoulders on postoperative radiographs. At the final follow-up, however, one shoulder with secondary synovial chondromatosis in the subacromial space showed recurrence of osteochondral lesions and acromial spur formation. The mean Constant score improved significantly from 53.0 points before resection to 76.0 points at a mean follow-up of 6.0 years (p = 0.002). On histopathological evaluation, one shoulder was diagnosed as having primary synovial chondromatosis, while nine shoulders had secondary synovial chondromatosis.
Conclusions: The present study showed that resection of shoulder osteochondral lesions successfully relieved the clinical symptoms and that primary synovial chondromatosis is less common than secondary synovial chondromatosis in the shoulder. Although most of the present osteochondral lesions were clinically determined to be primary chondromatosis, only one case was histopathologically categorized as primary synovial chondromatosis. These results suggest that histopathological identification is needed to differentiate between primary and secondary synovial chondromatosis.
Keywords: Chondromatosis; Osteochondromatosis; Shoulder; Synovial chondrometaplasia; Synovial osteochondromatosis.
Copyright © 2020 by The Korean Orthopaedic Association.
Conflict of interest statement
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Jaffe HL. Synovial chondromatosis and other benign articular tumors. In: Jaffe HL, editor. Tumors and tumorous conditions of the bones and joints. Philadelphia, PA: Lea & Febiger; 1958. pp. 558–567.
-
- Mussey RD, Jr, Henderson MS. Osteochondromatosis. J Bone Joint Surg Am. 1949;31A(3):619–627. - PubMed
-
- Milgram JW. The classification of loose bodies in human joints. Clin Orthop Relat Res. 1977;(124):282–291. - PubMed
-
- Ho YY, Choueka J. Synovial chondromatosis of the upper extremity. J Hand Surg Am. 2013;38(4):804–810. - PubMed
-
- Apte SS, Athanasou NA. An immunohistological study of cartilage and synovium in primary synovial chondromatosis. J Pathol. 1992;166(3):277–281. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
