

Assessment of surgical tumor-free resection margins in fresh squamous-cell carcinoma resection specimens of the tongue using a clinical MRI system
- PMID: 32119170
- PMCID: PMC7496932
- DOI: 10.1002/hed.26125
Assessment of surgical tumor-free resection margins in fresh squamous-cell carcinoma resection specimens of the tongue using a clinical MRI system
Abstract
Background: Current intraoperative methods of visual inspection and tissue palpation by the surgeon, and frozen section analysis cannot reliably prevent inadequate surgical margins in patients treated for oral squamous-cell carcinoma (OSCC). This study assessed feasibility of MRI for the assessment of surgical resection margins in fresh OSCC specimens.
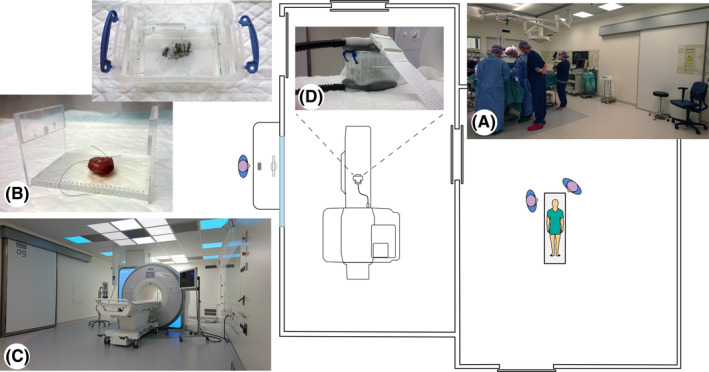
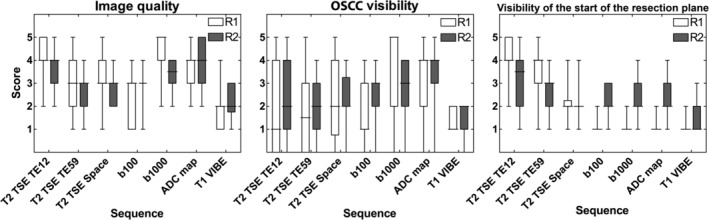
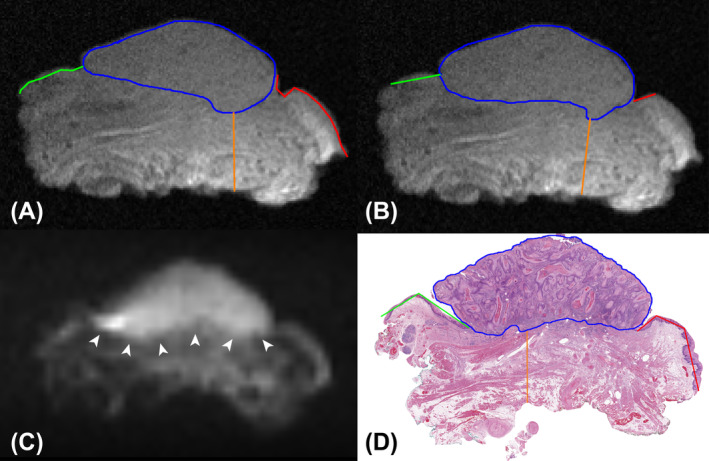
Methods: Ten consecutive tongue specimens containing OSCC were scanned using 3 T clinical whole-body MRI. Two radiologists independently annotated OSCC location and minimal tumor-free margins. Whole-mount histology was the reference standard.
Results: The positive predictive values (PPV) and negative predictive values (NPV) for OSCC localization were 96% and 75%, and 87% and 79% for reader 1 and 2, respectively. The PPV and NPV for identification of margins <5 mm were 38% and 91%, and 5% and 87% for reader 1 and 2, respectively.
Conclusions: MRI accurately localized OSCC with high inter-reader agreement in fresh OSCC specimens, but it seemed not yet feasible to accurately assess the surgical margin status.
Keywords: MRI; margins of excision; squamous cell carcinoma of head and neck; tongue neoplasms; whole mount histology.
© 2020 The Authors. Head & Neck published by Wiley Periodicals, Inc.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7‐30. - PubMed
-
- Bell RB, Kademani D, Homer L, Dierks EJ, Potter BE. Tongue cancer: is there a difference in survival compared with other subsites in the oral cavity? J Oral Maxillofac Surg. 2007;65(2):229‐236. - PubMed
-
- Yao M, Epstein JB, Modi BJ, Pytynia KB, Mundt AJ, Feldman LE. Current surgical treatment of squamous cell carcinoma of the head and neck. Oral Oncol. 2007;43(3):213‐223. - PubMed
-
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology, Head and Neck Cancer, Version 2.2013 [Internet]. https://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf. Accessed May 8, 2018.
-
- Slootweg PJ, Hordijk GJ, Schade Y, van Es RJJ, Koole R. Treatment failure and margin status in head and neck cancer. A critical view on the potential value of molecular pathology. Oral Oncol. 2002;38(5):500‐503. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
