

Ten-Year Update of a Randomized, Prospective Trial of Conventional Fractionated Versus Moderate Hypofractionated Radiation Therapy for Localized Prostate Cancer
- PMID: 32119599
- PMCID: PMC7238488
- DOI: 10.1200/JCO.19.01485
Ten-Year Update of a Randomized, Prospective Trial of Conventional Fractionated Versus Moderate Hypofractionated Radiation Therapy for Localized Prostate Cancer
Erratum in
-
Errata.J Clin Oncol. 2021 Jan 20;39(3):258. doi: 10.1200/JCO.20.03554. J Clin Oncol. 2021. PMID: 33450173 Free PMC article. No abstract available.
Abstract
Purpose: The previously published single institution randomized prospective trial failed to show superiority in the 5-year biochemical and/or clinical disease failure (BCDF) rate with moderate hypofractionated intensity-modulated radiation therapy (H-IMRT) versus conventionally fractionated IMRT (C-IMRT). We now present 10-year disease outcomes using updated risk groups and definitions of biochemical failure.
Methods: Men with protocol-defined intermediate- and high-risk prostate adenocarcinoma were randomly assigned to receive C-IMRT (76 Gy in 38 fractions) or H-IMRT (70.2 Gy in 26 fractions). Men with high-risk disease were all prescribed 24 months of androgen deprivation therapy (ADT) and had lymph node irradiation. Men with intermediate risk were prescribed 4 months of ADT at the discretion of the treating physician. The primary endpoint was cumulative incidence of BCDF. We compared disease outcomes and overall mortality by treatment arm, with sensitivity analyses for National Comprehensive Cancer Network (NCCN) risk group adjustment.
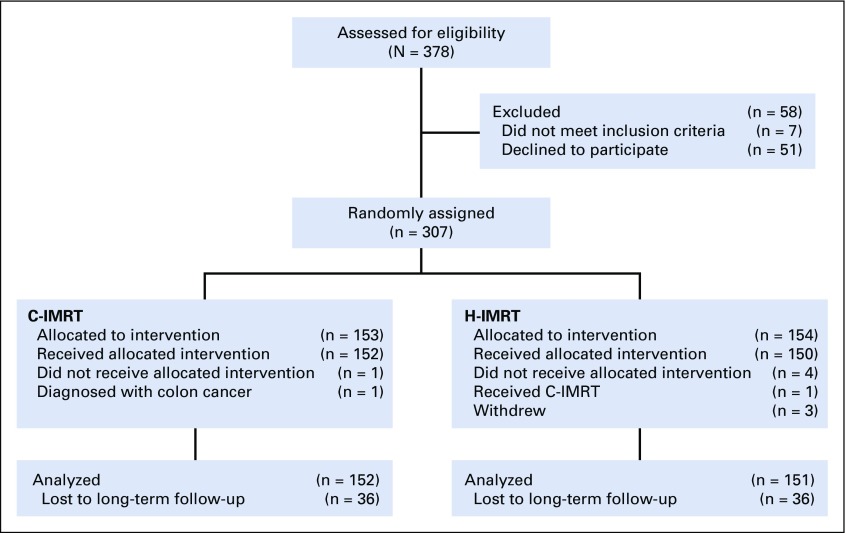
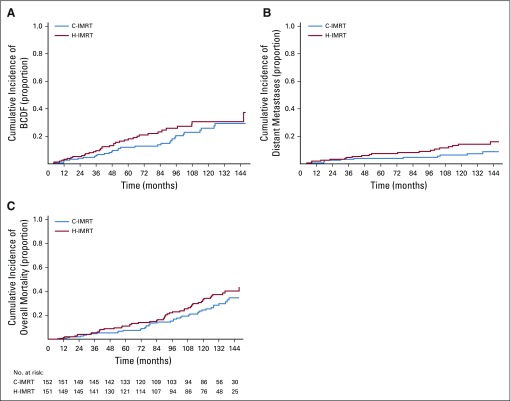
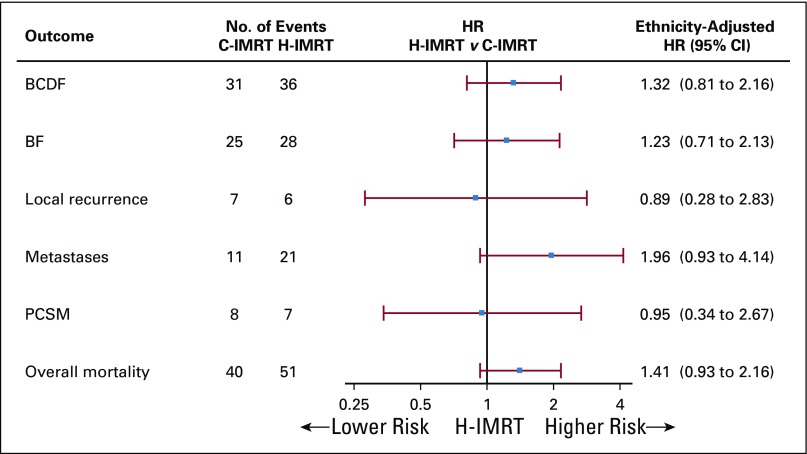
Results: Overall, 303 assessable men were randomly assigned to C-IMRT or H-IMRT. The median follow-up was 122.9 months. Per updated NCCN risk classification, there were 28 patients (9.2%) with low-risk, 189 (62.4%) with intermediate-risk, and 86 (28.4%) with high-risk prostate cancer. The arms were equally balanced for clinicopathologic factors, except that there were more black patients in the C-IMRT arm (17.8% v 7.3%; P = .02). There was no difference in ADT use (P = .56). The 10-year cumulative incidence of BCDF was 25.9% in the C-IMRT arm and was 30.6% in the H-IMRT arm (hazard ratio, 1.31; 95% CI, 0.82 to 2.11). The two arms also had similar cumulative 10-year rates of biochemical failure, prostate cancer-specific mortality, and overall mortality; however, the 10-year cumulative incidence of distant metastases was higher in the H-IMRT arm (rate difference, 7.8%; 95% CI, 0.7% to 15.1%).
Conclusion: H-IMRT failed to demonstrate superiority compared with C-IMRT in long-term disease outcomes.
Trial registration: ClinicalTrials.gov NCT00062309.
Conflict of interest statement
The contents of this publication are solely the responsibility of the authors and do not necessarily represent the official views of the National Cancer Institute, the National Institutes of Health, or Varian Medical Systems.
Figures
References
-
- Fitzmaurice C, Akinyemiju TF, Al Lami FH, et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2016: A systematic analysis for the Global Burden of Disease Study. JAMA Oncol. 2018;4:1553–1568. - PMC - PubMed
-
- Catton CN, Lukka H, Gu CS, et al. Randomized trial of a hypofractionated radiation regimen for the treatment of localized prostate cancer. J Clin Oncol. 2017;35:1884–1890. - PubMed
-
- Incrocci L, Wortel RC, Alemayehu WG, et al. Hypofractionated versus conventionally fractionated radiotherapy for patients with localised prostate cancer (HYPRO): Final efficacy results from a randomised, multicentre, open-label, phase 3 trial. Lancet Oncol. 2016;17:1061–1069. - PubMed
Publication types
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
