

Total resuscitative endovascular balloon occlusion of the aorta causes inflammatory activation and organ damage within 30 minutes of occlusion in normovolemic pigs
- PMID: 32122358
- PMCID: PMC7053141
- DOI: 10.1186/s12893-020-00700-3
Total resuscitative endovascular balloon occlusion of the aorta causes inflammatory activation and organ damage within 30 minutes of occlusion in normovolemic pigs
Abstract
Background: Resuscitative endovascular balloon occlusion of the aorta (REBOA) causes physiological, metabolic, end-organ and inflammatory changes that need to be addressed for better management of severely injured patients. The aim of this study was to investigate occlusion time-dependent metabolic, end-organ and inflammatory effects of total REBOA in Zone I in a normovolemic animal model.
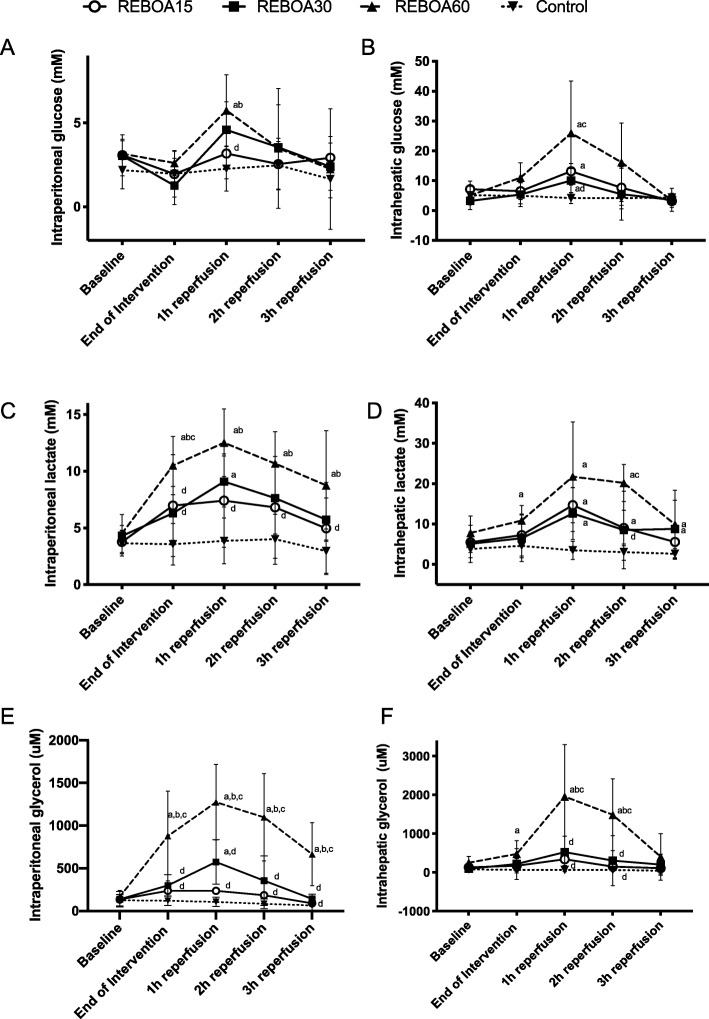
Methods: Twenty-four pigs (25-35 kg) were randomized to total occlusion REBOA in Zone I for either 15, 30, 60 min (REBOA15, REBOA30, and REBOA60, respectively) or to a control group, followed by 3-h reperfusion. Hemodynamic variables, metabolic and inflammatory response, intraperitoneal and intrahepatic microdialysis, and plasma markers of end-organ injuries were measured during intervention and reperfusion. Intestinal histopathology was performed.
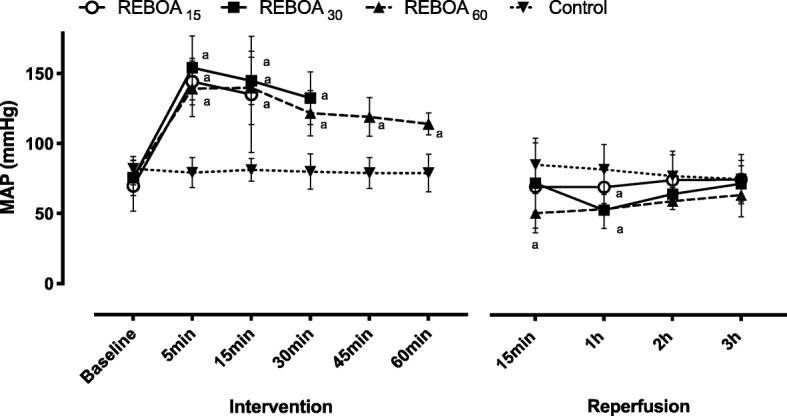
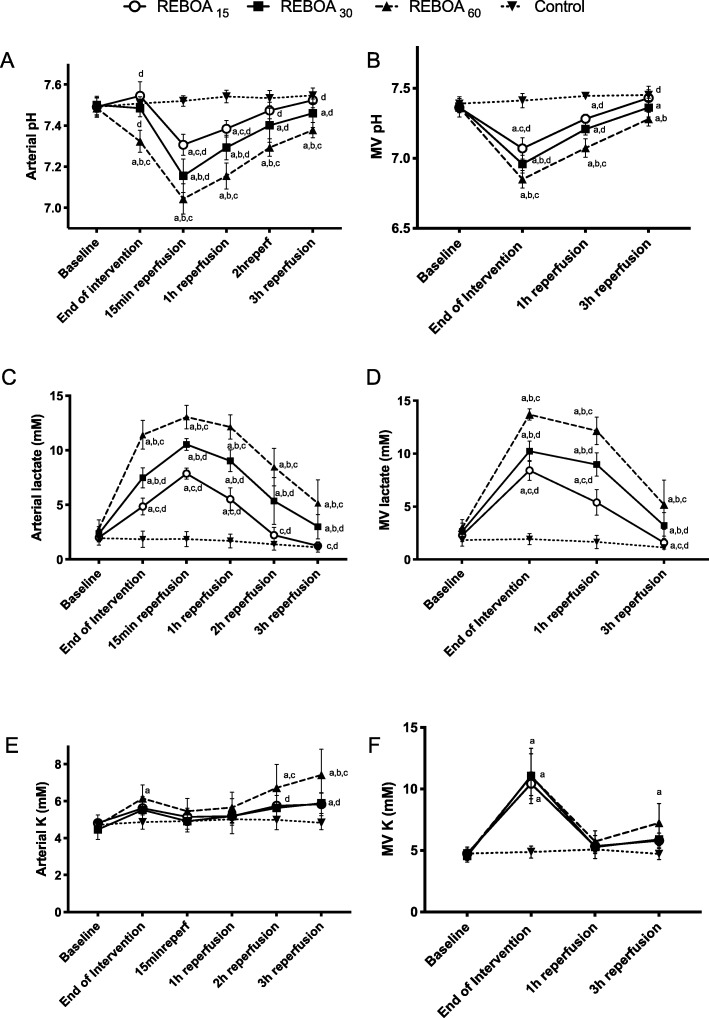
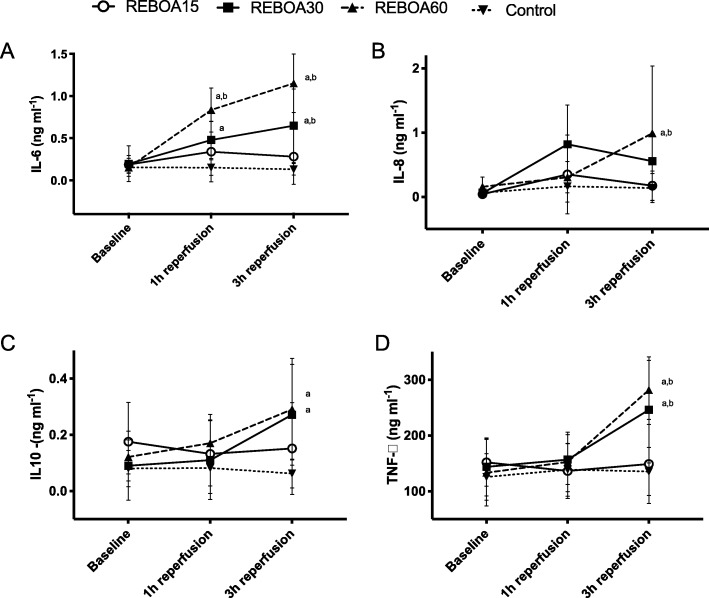
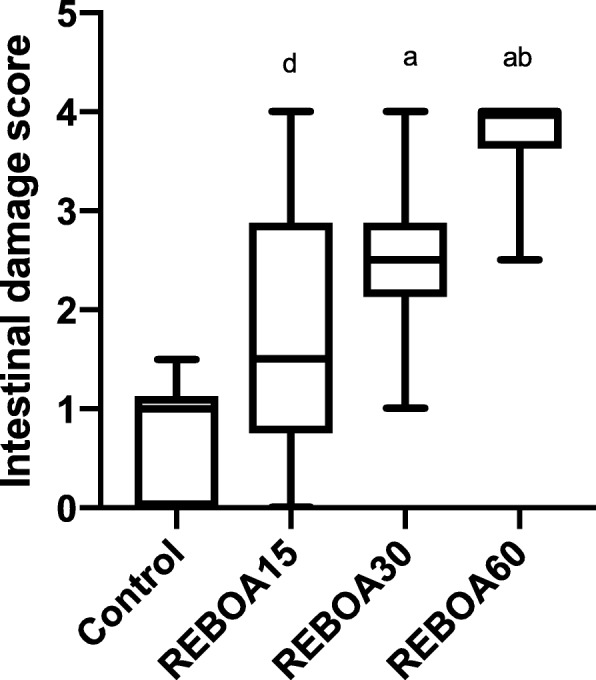
Results: Mean arterial pressure and cardiac output increased significantly in all REBOA groups during occlusion and blood flow in the superior mesenteric artery and urinary production subsided during intervention. Metabolic acidosis with increased intraperitoneal and intrahepatic concentrations of lactate and glycerol was most pronounced in REBOA30 and REBOA60 during reperfusion and did not normalize at the end of reperfusion in REBOA60. Inflammatory response showed a significant and persistent increase of pro- and anti-inflammatory cytokines during reperfusion in REBOA30 and was most pronounced in REBOA60. Plasma concentrations of liver, kidney, pancreatic and skeletal muscle enzymes were significantly increased at the end of reperfusion in REBOA30 and REBOA60. Significant intestinal mucosal damage was present in REBOA30 and REBOA60.
Conclusion: Total REBOA caused severe systemic and intra-abdominal metabolic disturbances, organ damage and inflammatory activation already at 30 min of occlusion.
Keywords: Ischemia reperfusion injury; Occlusion time; Organ damage; REBOA.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
A randomized porcine study of the hemodynamic and metabolic effects of combined endovascular occlusion of the vena cava and the aorta in normovolemia and in hemorrhagic shock.J Trauma Acute Care Surg. 2021 May 1;90(5):817-826. doi: 10.1097/TA.0000000000003098. J Trauma Acute Care Surg. 2021. PMID: 33496552 Free PMC article.
-
Extending the golden hour for Zone 1 resuscitative endovascular balloon occlusion of the aorta: Improved survival and reperfusion injury with intermittent versus continuous resuscitative endovascular balloon occlusion of the aorta of the aorta in a porcine severe truncal hemorrhage model.J Trauma Acute Care Surg. 2018 Aug;85(2):318-326. doi: 10.1097/TA.0000000000001964. J Trauma Acute Care Surg. 2018. PMID: 30080780
-
Endovascular variable aortic control (EVAC) versus resuscitative endovascular balloon occlusion of the aorta (REBOA) in a swine model of hemorrhage and ischemia reperfusion injury.J Trauma Acute Care Surg. 2018 Sep;85(3):519-526. doi: 10.1097/TA.0000000000002008. J Trauma Acute Care Surg. 2018. PMID: 30142105
-
Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) in the Management of Trauma Patients: A Systematic Literature Review.Am Surg. 2019 Jun 1;85(6):654-662. Am Surg. 2019. PMID: 31267908
-
Large Animal Models of Proximal Aortic Balloon Occlusion in Traumatic Hemorrhage: Review and Identification of Knowledge Gaps Relevant to Expanded Use.J Surg Res. 2019 Apr;236:247-258. doi: 10.1016/j.jss.2018.11.038. Epub 2018 Dec 21. J Surg Res. 2019. PMID: 30694763 Review.
Cited by
-
A clinical study of the hemodynamic and metabolic effects of Zone 3 REBOA for sacral and pelvic tumor resections.BMC Surg. 2022 Jun 27;22(1):246. doi: 10.1186/s12893-022-01694-w. BMC Surg. 2022. PMID: 35761238 Free PMC article.
-
Complications associated with the use of resuscitative endovascular balloon occlusion of the aorta (REBOA): an updated review.Trauma Surg Acute Care Open. 2024 Feb 7;9(1):e001267. doi: 10.1136/tsaco-2023-001267. eCollection 2024. Trauma Surg Acute Care Open. 2024. PMID: 38347890 Free PMC article. Review.
-
Hydrogen gas inhalation therapy may not work sufficiently to mitigate oxidative stress induced with REBOA.Sci Rep. 2024 Dec 30;14(1):32128. doi: 10.1038/s41598-024-83934-y. Sci Rep. 2024. PMID: 39739016 Free PMC article.
-
Application of resuscitative endovascular balloon occlusion in post-transplant mycotic hepatic artery pseudoaneurysm rupture in the setting of Aspergillus Constellatus bacteremia.Ann Hepatobiliary Pancreat Surg. 2021 Feb 28;25(1):126-131. doi: 10.14701/ahbps.2021.25.1.126. Ann Hepatobiliary Pancreat Surg. 2021. PMID: 33649265 Free PMC article.
-
Impact of resuscitative endovascular balloon occlusion of the aorta on gastrointestinal function with a matched cohort study.Trauma Surg Acute Care Open. 2024 Jan 30;9(1):e001239. doi: 10.1136/tsaco-2023-001239. eCollection 2024. Trauma Surg Acute Care Open. 2024. PMID: 38298820 Free PMC article.
References
-
- Horer TM, Skoog P, Pirouzram A, Nilsson KF, Larzon T. A small case series of aortic balloon occlusion in trauma: lessons learned from its use in ruptured abdominal aortic aneurysms and a brief review. Eur J Trauma Emerg Surg. 2015. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
