

Combined surgery with 3-in-1 osteosynthesis in congenital pseudarthrosis of the tibia with intact fibula
- PMID: 32122367
- PMCID: PMC7053109
- DOI: 10.1186/s13023-020-1330-z
Combined surgery with 3-in-1 osteosynthesis in congenital pseudarthrosis of the tibia with intact fibula
Abstract
Background: Re-fracture is the most serious complication in congenital pseudarthrosis of the tibia (CPT). There are reports that children with small cross-sectional areas in the sections of the pseudarthrosis are more prone to re-fracture. Presently, preventing complications is a challenge. Increasing the cross-sectional area in healed segments may reduce the incidence of re-fracture.
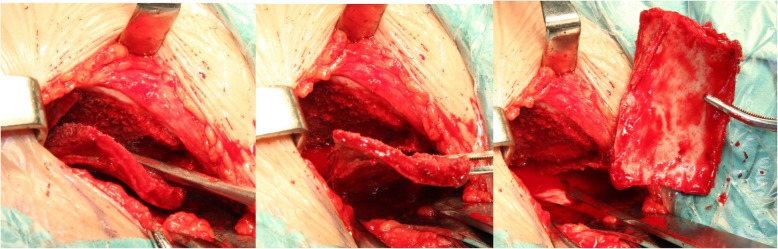
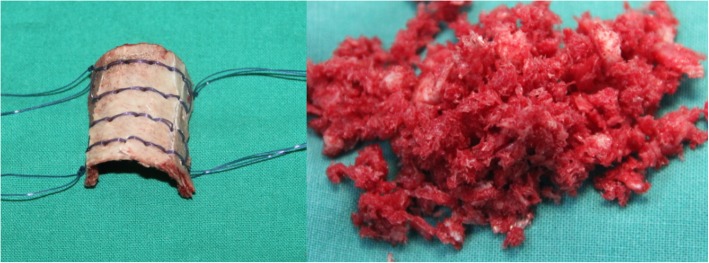
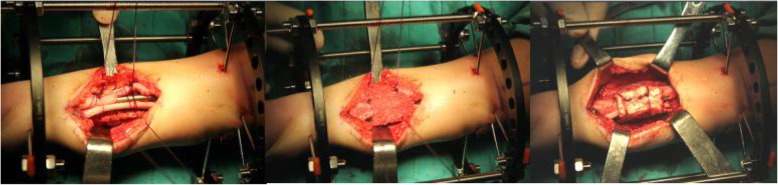
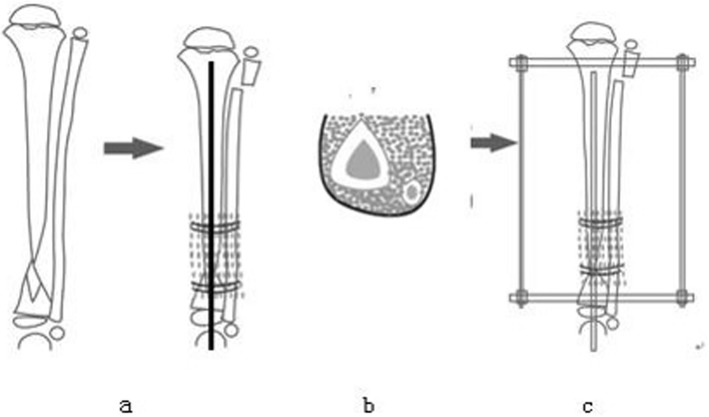
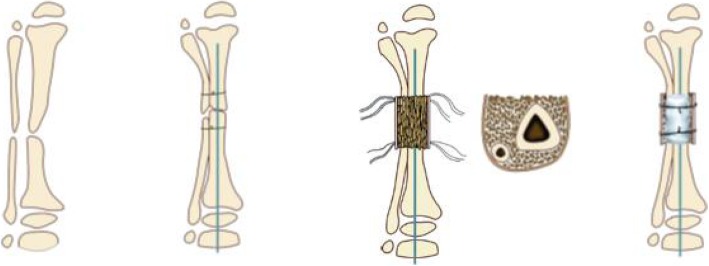
Purpose: To elucidate the indications, surgical technique, and outcomes of combined surgery and 3-in-1 osteosynthesis in CPT with intact fibula.
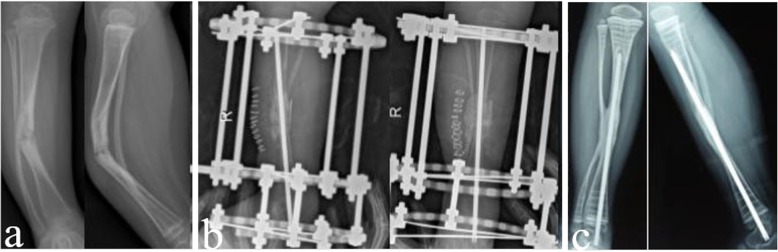
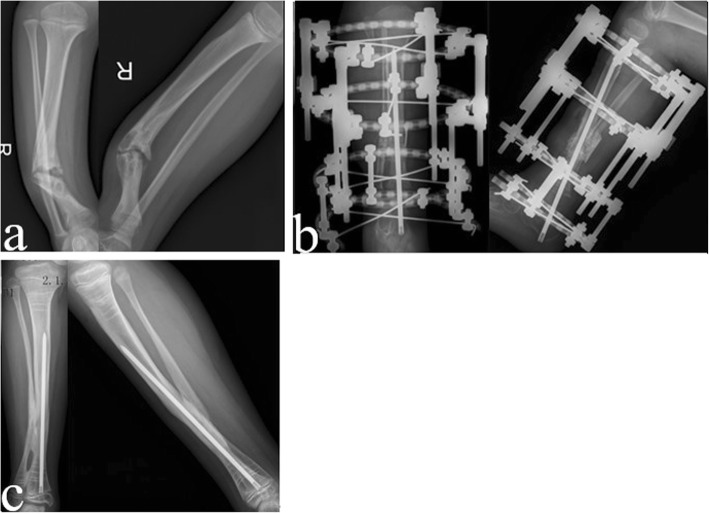
Methods: We retrospectively assessed 17 patients with Crawford Type IV CPT with intact fibula (Type A) who were treated with combined surgical technique and 3-in-1 osteosynthesis between March 2014 and August 2015. The average age of the patients at the time of surgery was 3 years. Incidence of re-fracture, ankle valgus, proximal tibial valgus, and limb length discrepancy (LLD) were investigated over an average follow-up time of 47 months.
Results: Primary union was achieved in all patients. The average time for primary union was 4.9 months. Fifteen (88%) cases showed LLD with an average limb length of 1.6 cm; 6 (35%) cases exhibited tibial valgus with an average tibial valgus deformity of 7.8°; 2 cases had ankle valgus, wherein the ankle valgus deformity was 12° in one and 17° in another; and the cross-sectional area of the bone graft was enlarged to 1.74 times that of the tibia shaft. No case had re-fracture during the follow-up period. Movement of the ankle joint was restored in 16 patients with an average dorsiflexion of 22° and an average plantar flexion of 41°; the function of the ankle joint was normal. One patient had plantar flexion of 20° but did not have dorsiflexion.
Conclusion: Combined surgical technique with 3-in-1 osteosynthesis, which is primarily considered for bone union with a large cross-sectional area, results in a high primary union rate. This can provide satisfactory results in short-term follow-up when treating CPT with intact fibula (Type A).
Keywords: 3-in-1 osteosynthesis; Congenital pseudarthrosis of tibia; Fibula intact.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Paley Dror. Bone Grafting. 2012. Congenital Pseudarthrosis of the Tibia: Combined Pharmacologic and Surgical Treatment Using Biphosphonate Intravenous Infusion and Bone Morphogenic Protein with Periosteal and Cancellous Autogenous Bone Grafting, Tibio-Fibular Cross Union, Intramedullary.
-
- Zhu GH, Mei HB, He RG. Combination of intramedullary rod, wrapping bone grafting and Ilizarov's fixator for the treatment of Crawford type IV congenital pseudarthrosis of the tibia: mid-term follow up of 56 cases [J] BMC Musculoskelet Disord. 2016;17(1):443. doi: 10.1186/s12891-016-1295-1. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
