

Free-breathing dynamic contrast-enhanced magnetic resonance of interstitial lung fibrosis
- PMID: 32126265
- PMCID: PMC7986483
- DOI: 10.1016/j.mri.2020.02.014
Free-breathing dynamic contrast-enhanced magnetic resonance of interstitial lung fibrosis
Abstract
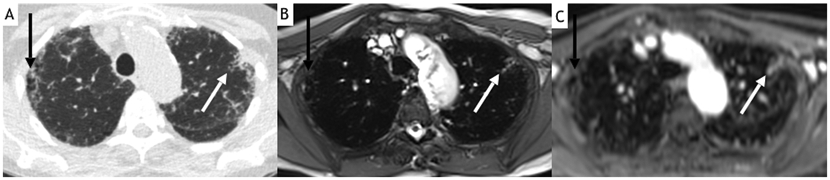
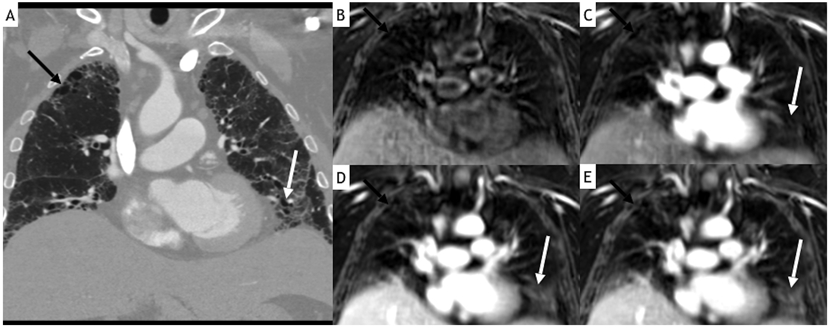
Purpose: Computed tomography (CT) imaging is the standard to assess interstitial lung disease. Magnetic resonance (MR) is potentially advantageous due to superior tissue characterization and better assessment of blood flow dynamics. This study aimed to evaluate idiopathic pulmonary fibrosis (IPF) using prototype 4D Stack of Stars GRE (StarVIBE) MR and compare it to CT.
Method: This IRB-approved prospective study included 13 patients [5F:8M; average age 66 ± 8.1 years] with pulmonary fibrosis, and 12 healthy controls [3F:9M; average age 55 ± 3.6 years]. MR of the chest included noncontrast steady-state free precession imaging (SSFP) and free-breathing 4D StarVIBE sequence with intravenous contrast administration up to 160 s. The images were assessed for quality and artifacts. The image resolution was evaluated based on the visibility of the smallest bronchi, vessels, lymph nodes, and pleural fissures. Independent assessment of reticulation, ground-glass opacity, and traction bronchiectasis was performed and compared to CT.
Results: The StarVIBE images had fewer artifacts and higher spatial resolution. The findings associated with IPF were significantly better seen with StarVIBE, with superior CT correlation.
Conclusion: Contrast-enhanced free-breathing StarVIBE MR can generate high quality images with good correlation to CT in patients with IPF, and with high spatial and temporal resolution to generate rapid sequential dynamic images.
Keywords: Interstitial lung disease; Magnetic resonance imaging; Pulmonary fibrosis; StarVIBE.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of competing interest R.S. is an employee of Siemens Healthcare. The other authors report no potential conflicts of interest.
Figures
References
-
- Raghu G, Collard HR, Egan JJ, Martinez FJ, Behr J, Brown KK, Colby TV, Cordier JF, Flaherty KR, Lasky JA, Lynch DA, Ryu JH, Swigris JJ, Wells AU, Ancochea J, Bouros D, Carvalho C, Costabel U, Ebina M, Hansell DM, Johkoh T, Kim DS, King TE, Kondoh Y, Myers J, Müller NL, Nicholson AG, Richeldi L, Selman M, Dudden RF, Griss BS, Protzko SL, Schünemann HJ, An Official ATS/ERS/JRS/ALAT Statement: Idiopathic pulmonary fibrosis: Evidence-based guidelines for diagnosis and management, Am. J. Respir. Crit. Care Med 183 (2011) 788–824. doi:10.1164/rccm.2009-040GL. - DOI - PMC - PubMed
-
- Lynch DA, Sverzellati N, Travis WD, Brown KK, Colby TV, Galvin JR, Goldin JG, Hansell DM, Inoue Y, Johkoh T, Nicholson AG, Knight SL, Raoof S, Richeldi L, Ryerson CJ, Ryu JH, Wells AU, Diagnostic criteria for idiopathic pulmonary fibrosis: a Fleischner Society White Paper, Lancet Respir. Med 6 (2018) 138–153. doi:10.1016/S2213-2600(17)30433-2. - DOI - PubMed
-
- Raghu G, Remy-Jardin M, Myers JL, Richeldi L, Ryerson CJ, Lederer DJ, Behr J, Cottin V, Danoff SK, Morell F, Flaherty KR, Wells A, Martinez FJ, Azuma A, Bice TJ, Bouros D, Brown KK, Collard HR, Duggal A, Galvin L, Inoue Y, Jenkins RG, Johkoh T, Kazerooni EA, Kitaichi M, Knight SL, Mansour G, Nicholson AG, Pipavath SNJ, Buendía-Roldán I, Selman M, Travis WD, Walsh SLF, Wilson KC, Diagnosis of Idiopathic Pulmonary Fibrosis. An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline, Am. J. Respir. Crit. Care Med 198 (2018) e44–e68. doi:10.1164/rccm.201807-1255ST. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
