

Opportunities for machine learning to improve surgical ward safety
- PMID: 32127174
- PMCID: PMC7673643
- DOI: 10.1016/j.amjsurg.2020.02.037
Opportunities for machine learning to improve surgical ward safety
Abstract
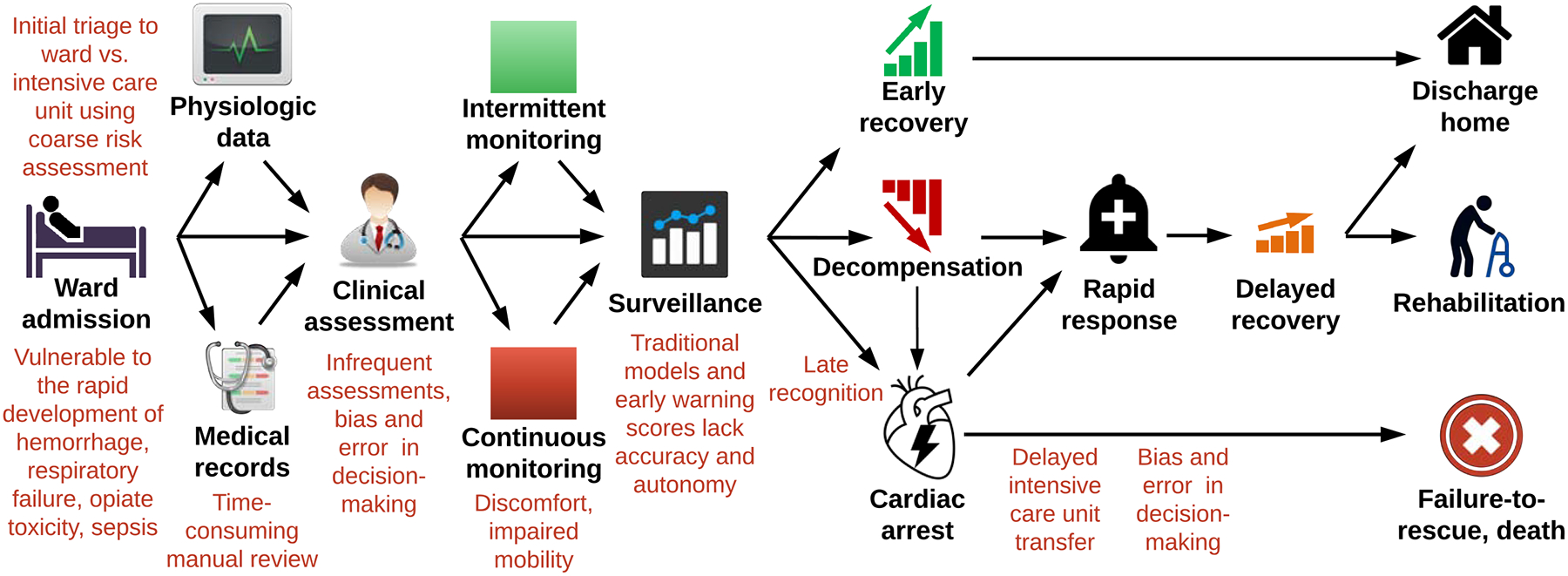
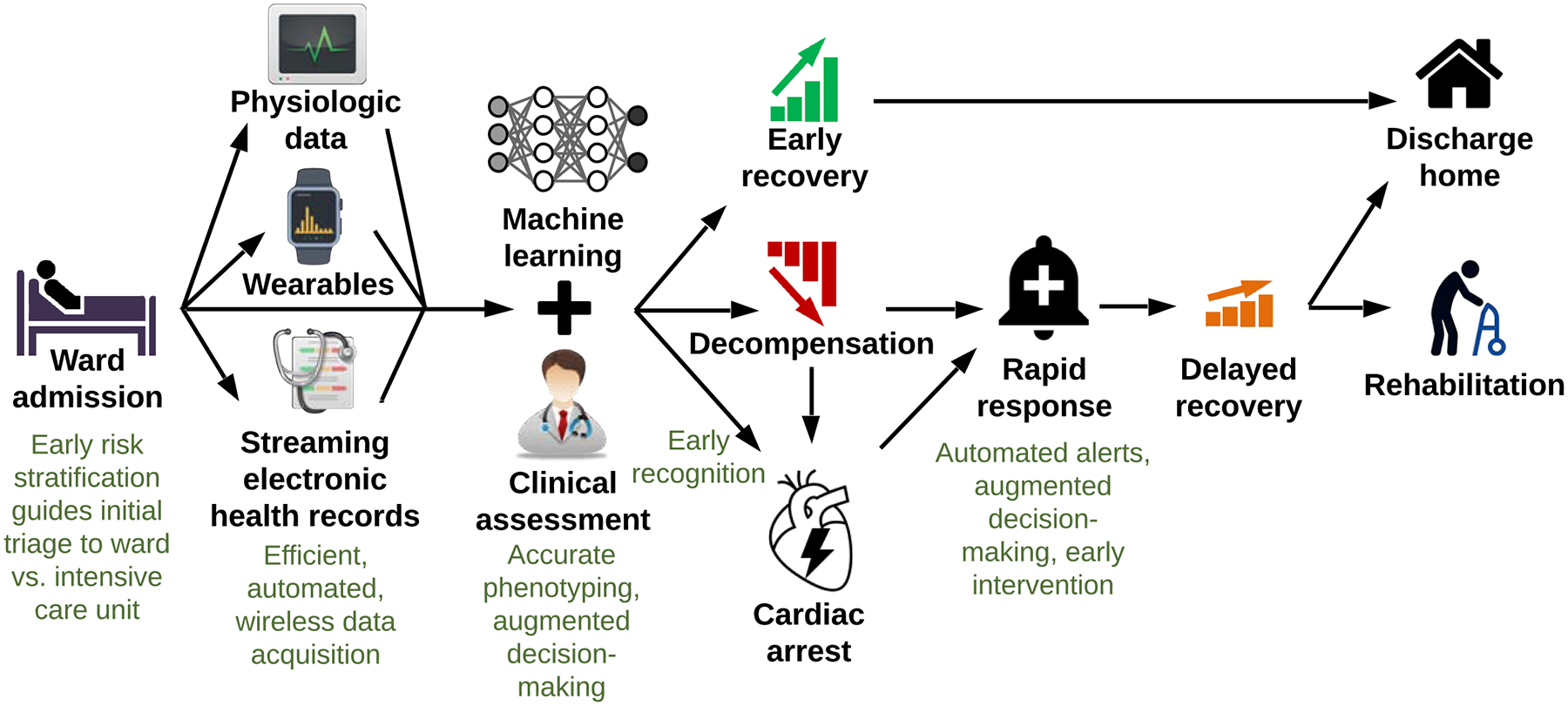
Background: Delayed recognition of decompensation and failure-to-rescue on surgical wards are major sources of preventable harm. This review assimilates and critically evaluates available evidence and identifies opportunities to improve surgical ward safety.
Data sources: Fifty-eight articles from Cochrane Library, EMBASE, and PubMed databases were included.
Conclusions: Only 15-20% of patients suffering ward arrest survive. In most cases, subtle signs of instability often occur prior to critical illness and arrest, and underlying pathology is reversible. Coarse risk assessments lead to under-triage of high-risk patients to wards, where surveillance for complications depends on time-consuming manual review of health records, infrequent patient assessments, prediction models that lack accuracy and autonomy, and biased, error-prone decision-making. Streaming electronic heath record data, wearable continuous monitors, and recent advances in deep learning and reinforcement learning can promote efficient and accurate risk assessments, earlier recognition of instability, and better decisions regarding diagnosis and treatment of reversible underlying pathology.
Keywords: Cardiac arrest; Decompensation; Deterioration; Machine learning; Surgery; Ward.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors have no relevant conflicts of interest. AB and PR were supported by R01 GM110240 from the NIGMS. AB was supported by P50 GM-111152 from the NIGMS. PR was supported by CAREER award, NSF-IIS 1750192, from the National Science Foundation (NSF), Division of Information and Intelligent Systems (IIS). PTJ was supported by R01GM114290 from the NIGMS. TJL was supported by a post-graduate training grant (T32 GM-008721) in burns, trauma, and perioperative injury from the NIGMS.
Figures
References
-
- Skogvoll E, Isern E, Sangolt GK, Gisvold SE. In-hospital cardiopulmonary resuscitation. 5 years’ incidence and survival according to the Utstein template. Acta Anaesthesiol Scand, 1999. February;43(2):177–84. - PubMed
-
- Sandroni C, Nolan J, Cavallaro F, Antonelli M. In-hospital cardiac arrest: incidence, prognosis and possible measures to improve survival. Intensive Care Med, 2007. February;33(2):237–45. - PubMed
-
- Franklin C, Mathew J. Developing strategies to prevent inhospital cardiac arrest: analyzing responses of physicians and nurses in the hours before the event. Crit Care Med, 1994. February;22(2):244–7. - PubMed
-
- Berlot G, Pangher A, Petrucci L, et al. Anticipating events of in-hospital cardiac arrest. Eur J Emerg Med, 2004. February;11(1):24–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
