

Lower DLco% identifies exercise pulmonary hypertension in patients with parenchymal lung disease referred for dyspnea
- PMID: 32128158
- PMCID: PMC7031800
- DOI: 10.1177/2045894019891912
Lower DLco% identifies exercise pulmonary hypertension in patients with parenchymal lung disease referred for dyspnea
Abstract
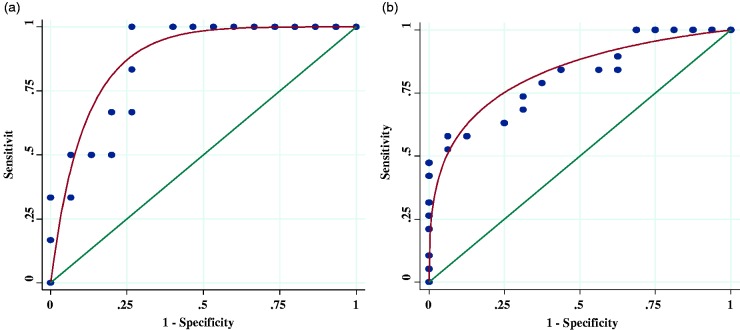
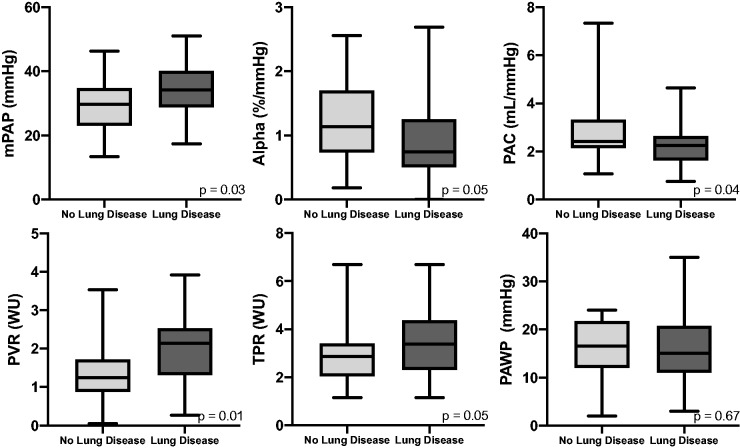
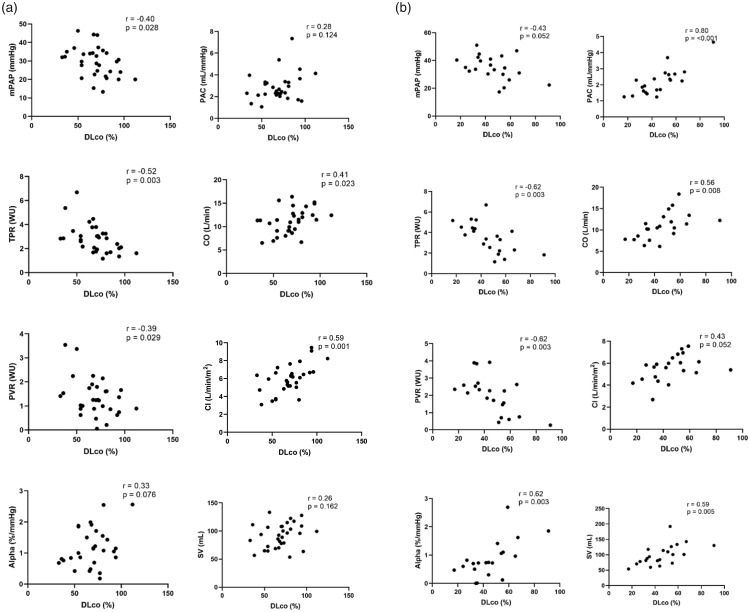
Exercise pulmonary hypertension is an underappreciated form of physical limitation related to early pulmonary vascular disease. A low diffusing capacity of lungs for carbon monoxide (DLco) can be seen in patients with resting pulmonary hypertension as well as parenchymal lung disease. It remains unclear whether low DLco% identifies early pulmonary vascular disease. We hypothesize that a reduced DLco% differentiates the presence of exercise pulmonary hypertension in patients with parenchymal lung disease. Fifty-six patients referred for unexplained exertional dyspnea with pulmonary function tests within six months of hemodynamic testing underwent exercise right heart catheterization. Exclusion criteria included resting pulmonary arterial or venous hypertension. Receiver operator characteristic curve determined the optimal DLco% cutoffs based on the presence or absence of parenchymal lung disease. Twenty-one (37%) patients had parenchymal lung disease, most common manifesting as chronic obstructive lung disease or interstitial lung disease. In patients with parenchymal lung disease, a DLco of 46% demonstrated 100% sensitivity and 73% specificity for detecting exercise pulmonary hypertension. In patients without parenchymal lung disease, a DLco of 73% demonstrated 58% sensitivity and 94% specificity for detecting exercise pulmonary hypertension. In both cohorts, DLco% below the optimum cutoffs were associated with higher peak mean pulmonary arterial pressure and peak total pulmonary resistance consistent with the hemodynamic definition of exercise pulmonary hypertension. Patients with a DLco < 46% were more often treated with pulmonary vasodilators and had a trend to higher mortality and lung transplant. DLco% is a simple non-invasive screening test for the presence of exercise pulmonary hypertension in our mixed referral population with progressive exertional dyspnea. DLco < 46% with parenchymal lung disease and DLco < 73% without parenchymal lung disease may play a role in differentiating the presence of pulmonary vascular disease prior to invasive hemodynamic testing.
Keywords: chronic obstructive lung disease (COPD); exercise pulmonary hypertension; hemodynamics; interstitial lung disease; pulmonary arterial hypertension.
© The Author(s) 2020.
Figures
References
-
- Herve P, Lau EM, Sitbon O, et al. Criteria for diagnosis of exercise pulmonary hypertension. Eur Respir J 2015; 46: 728–737. - PubMed
-
- Lewis GD, Bossone E, Naeije R, et al. Pulmonary vascular hemodynamic response to exercise in cardiopulmonary diseases. Circulation 2013; 128: 1470–1479. - PubMed
-
- Lau EM, Chemla D, Godinas L, et al. Loss of vascular distensibility during exercise is an early hemodynamic marker of pulmonary vascular disease. Chest 2016; 149: 353–361. - PubMed
-
- Godinas L, Lau EM, Chemla D, et al. Diagnostic concordance of different criteria for exercise pulmonary hypertension in subjects with normal resting pulmonary artery pressure. Eur Respir J 2016; 48: 254–257. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
