

Machine learning in prediction of individual patient readmissions for elective carotid endarterectomy, aortofemoral bypass/aortic aneurysm repair, and femoral-distal arterial bypass
- PMID: 32128209
- PMCID: PMC7036506
- DOI: 10.1177/2050312120909057
Machine learning in prediction of individual patient readmissions for elective carotid endarterectomy, aortofemoral bypass/aortic aneurysm repair, and femoral-distal arterial bypass
Abstract
Objective: Early hospital readmissions have been rising and are increasingly used for public reporting and pay-for-performance. The readmission problem is fundamentally different in surgical patients compared with medical patients. There is an opportunity to intervene preoperatively to decrease the risk of readmission postoperatively.
Methods: A predictive model of 90-day hospital readmission for patients undergoing elective carotid endarterectomy, aortofemoral bypass/aortic aneurysm repair, and femoral-distal arterial bypass was developed using data from the Healthcare Cost and Utilization Project State Inpatient Database for Florida State. The model training followed a nested resampling method with subsampling to increase execution speed and reduce overfitting. The following predictors were used: age, gender, race, median household income, primary expected payer, patient location, admission type, Elixhauser-van Walraven Comorbidity Index, Charlson comorbidity score, main surgical procedure, length of stay, disposition of the patient at discharge, period of the year, hospital volume, and surgeon volume.
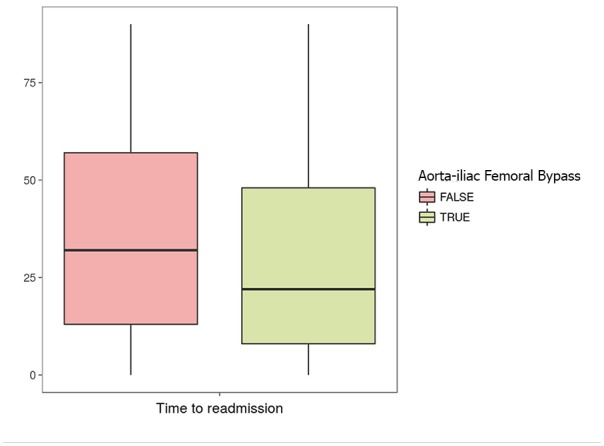
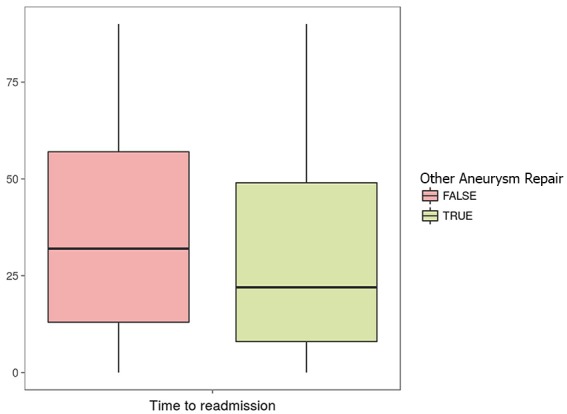
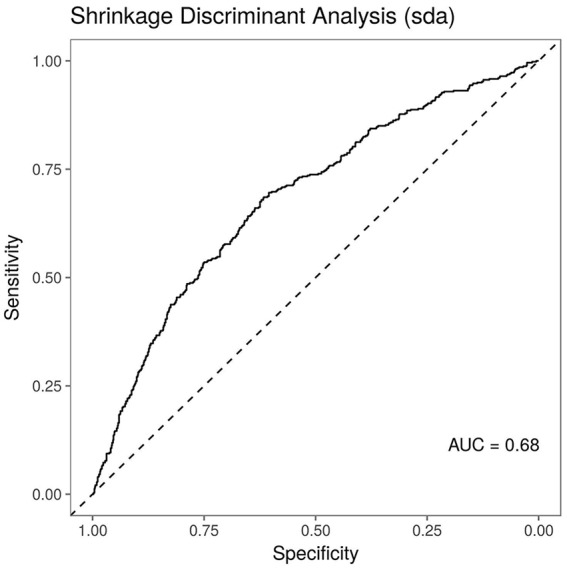
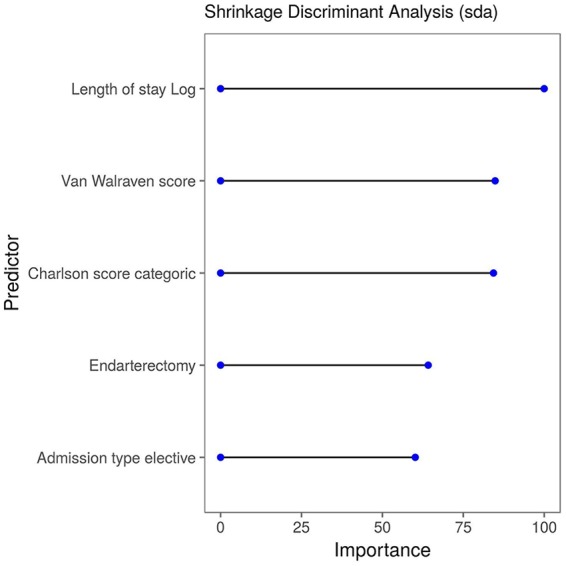
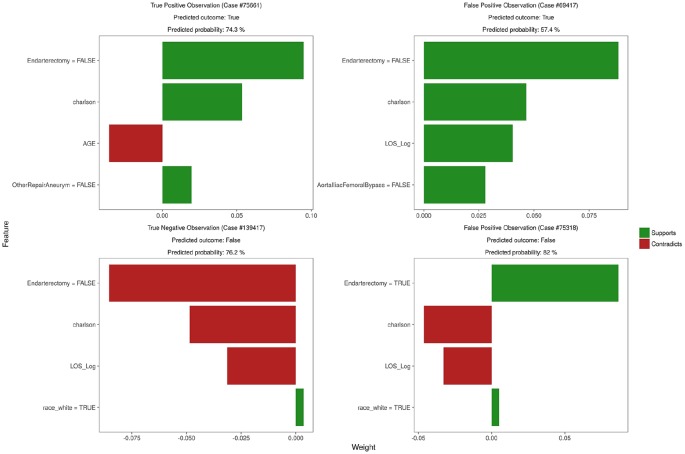
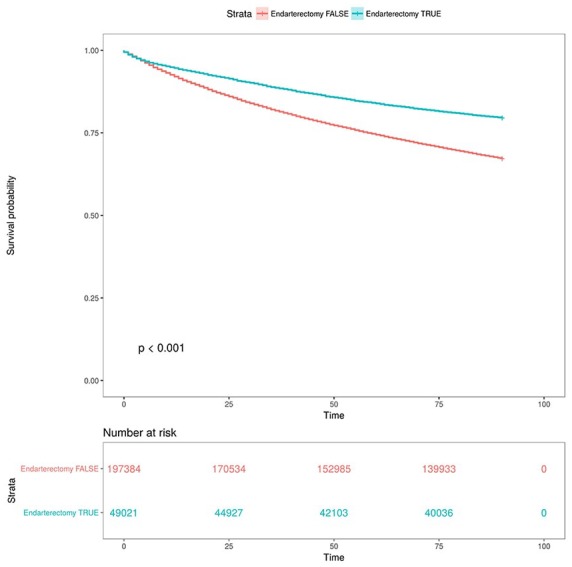
Results: Our sample comprised data on 246,405 patients, of whom 30.3% were readmitted within 90 days. Readmitted patients were more likely to be admitted via emergency (47.2% vs 30%), included a higher percentage with a Charlson score greater than 3 (35.8% vs 18.7%), had a higher mean van Walraven score (8.32 vs 5.34), and had a higher mean length of hospital stay (6.59 vs 3.51). Endarterectomy was the most common procedure, accounting for 19.9% of all procedures. When predicting 90-day readmission, Shrinkage Discriminant Analysis was the best performing model (area under the curve = 0.68). Important variables for the best predictive model included length of stay in the hospital, comorbidity scores, endarterectomy procedure, and elective admission type. The survival analysis for the time to readmission after the surgical procedures demonstrated that the hazard ratios were higher for subjects who presented Charlson comorbidity score above three (2.29 (2.26, 2.33)), patients transferred to a short-term hospital (2.4 (2.23, 2.59)), home healthcare (1.64 (1.61, 1.68)), other type of facility (2.59 (2.54, 2.63)) or discharged against medical advice (2.06 (1.88, 2.26)), and those with greater length of stay (1.89 (1.86, 1.91)).
Conclusion: The model stratifies readmission risk on the basis of vascular procedure type, which suggests that attempts to decrease vascular readmission should focus on emergency procedures. Given the current focus on readmissions and increasing pressure to prevent unplanned readmissions, this score stratifies patients by readmission risk, providing an additional resource to identify and prevent unnecessary readmissions.
Keywords: Aneurysm; carotid treatment; disease; outcome analysis; peripheral arterial occlusive; practice issues; vascular centers.
© The Author(s) 2020.
Conflict of interest statement
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Unplanned 30-Day Readmission Rates for Autosomal Dominant Polycystic Kidney Disease: Insight from the Nationwide Readmissions Database.Blood Purif. 2022 Nov 1:1-9. doi: 10.1159/000526923. Online ahead of print. Blood Purif. 2022. PMID: 36318891
-
Readmissions after complex aneurysm repair are frequent, costly, and primarily at nonindex hospitals.J Vasc Surg. 2014 Dec;60(6):1429-37. doi: 10.1016/j.jvs.2014.08.092. Epub 2014 Oct 12. J Vasc Surg. 2014. PMID: 25316154
-
Unplanned readmissions after vascular surgery.J Vasc Surg. 2014 Feb;59(2):473-82. doi: 10.1016/j.jvs.2013.09.002. Epub 2013 Nov 15. J Vasc Surg. 2014. PMID: 24239519
-
Temporal Trends and Predictors of Thirty-Day Readmissions and Emergency Department Visits Following Total Knee Arthroplasty in Ontario Between 2003 and 2016.J Arthroplasty. 2020 Feb;35(2):364-370. doi: 10.1016/j.arth.2019.09.015. Epub 2019 Sep 14. J Arthroplasty. 2020. PMID: 31732370 Review.
-
Overview of Clinical Conditions With Frequent and Costly Hospital Readmissions by Payer, 2018.2021 Jul 20. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2006 Feb–. Statistical Brief #278. 2021 Jul 20. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2006 Feb–. Statistical Brief #278. PMID: 34460186 Free Books & Documents. Review.
Cited by
-
Predictive modeling for identification of older adults with high utilization of health and social services.Scand J Prim Health Care. 2024 Dec;42(4):609-616. doi: 10.1080/02813432.2024.2372297. Epub 2024 Jul 3. Scand J Prim Health Care. 2024. PMID: 38958358 Free PMC article.
References
-
- Rosen AK, Chen Q, Shin MH, et al. Medical and surgical readmissions in the Veterans Health Administration: what proportion are related to the index hospitalization. Med Care 2014; 52(3): 243–249. - PubMed
LinkOut - more resources
Full Text Sources
