

Risk factors of perioperative mortality from complicated peptic ulcer disease in Africa: systematic review and meta-analysis
- PMID: 32128227
- PMCID: PMC7039611
- DOI: 10.1136/bmjgast-2019-000350
Risk factors of perioperative mortality from complicated peptic ulcer disease in Africa: systematic review and meta-analysis
Abstract
Introduction: In 2013, peptic ulcer disease (PUD) caused over 300 000 deaths globally. Low-income and middle-income countries are disproportionately affected. However, there is limited information regarding risk factors of perioperative mortality rates in these countries.
Objective: To assess perioperative mortality rates from complicated PUD in Africa and associated risk factors.
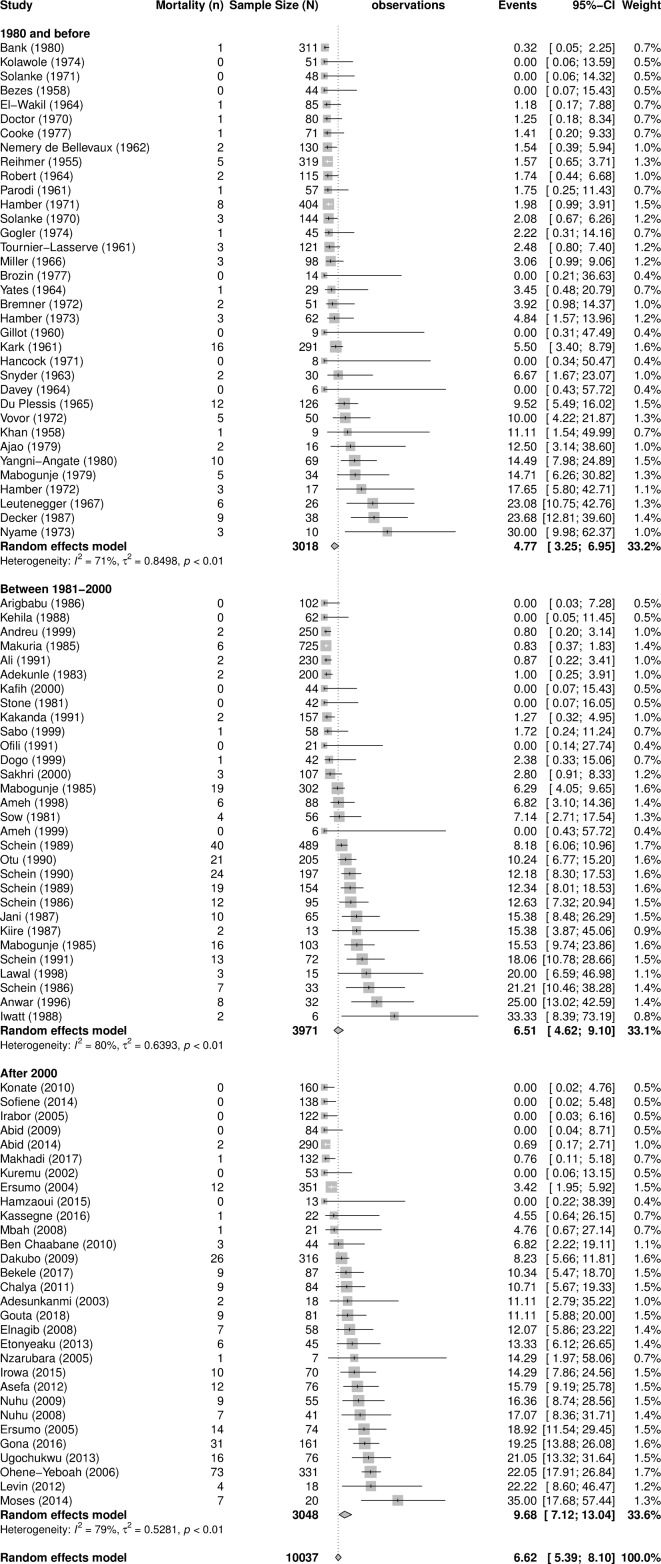
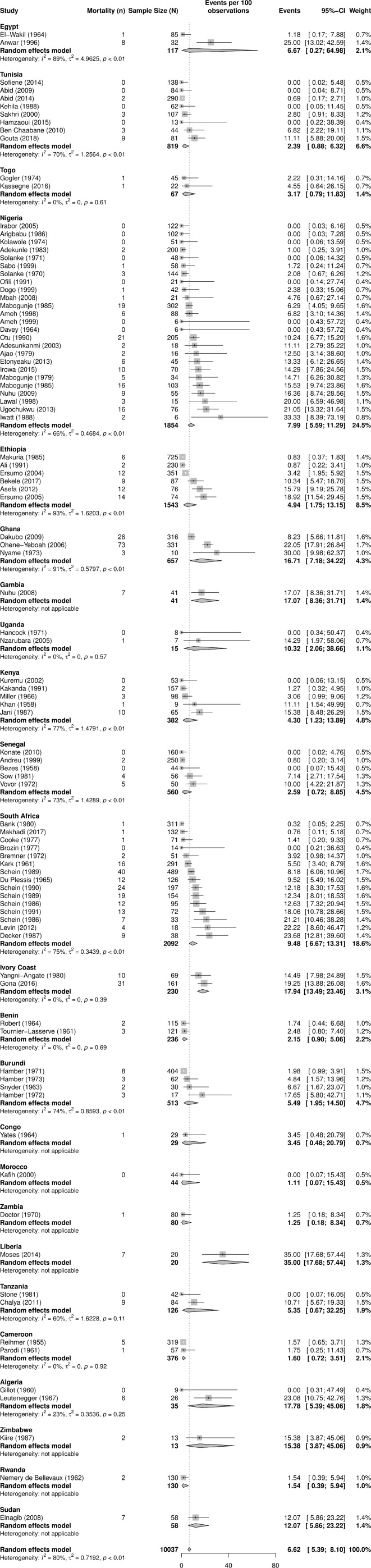
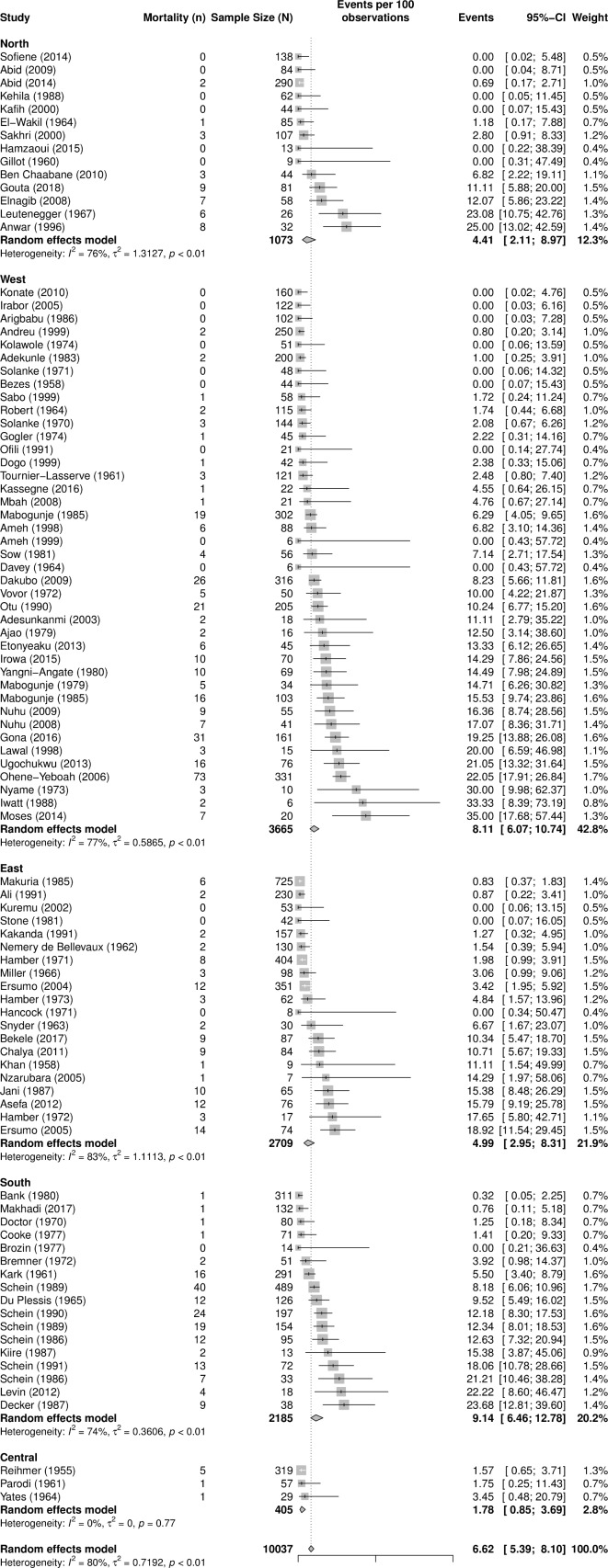
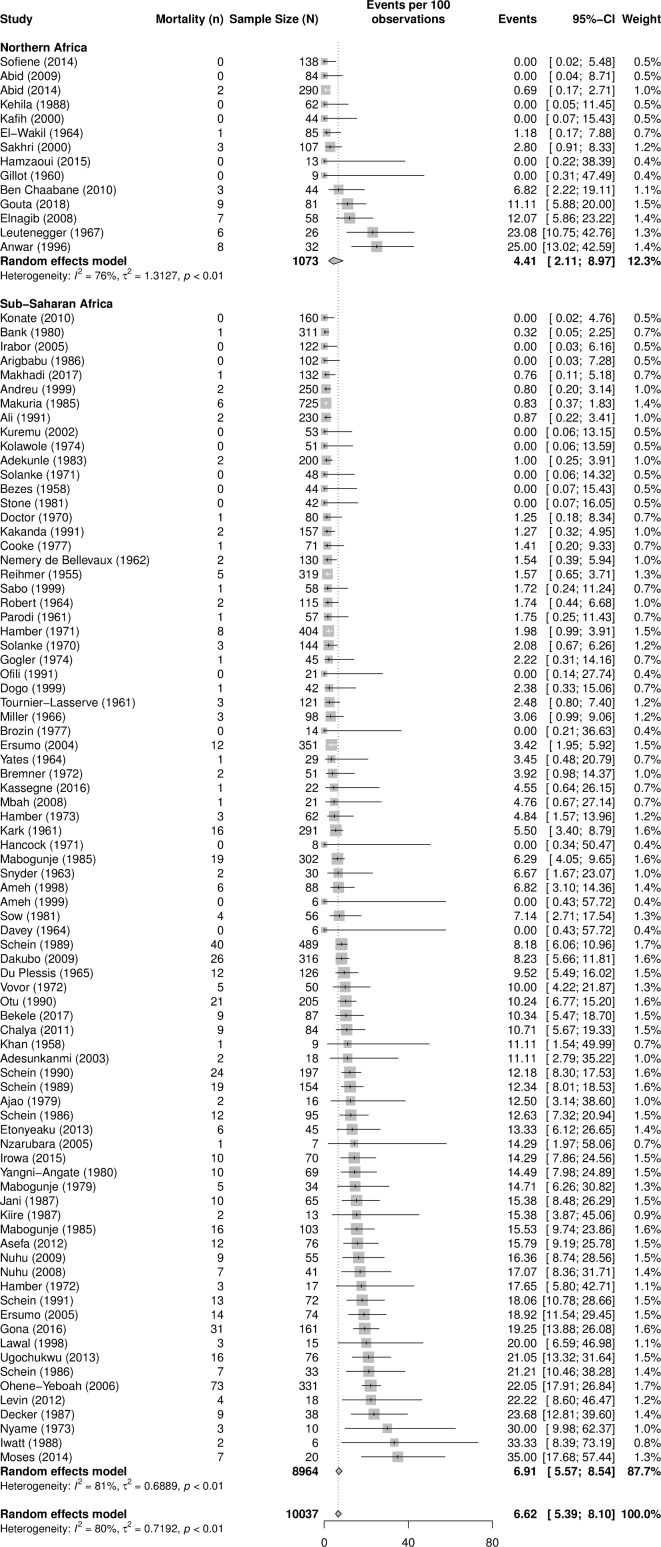
Design: We performed a systematic review and a random-effect meta-analysis of literature describing surgical management of complicated PUD in Africa. We used subgroup analysis and meta-regression analyses to investigate sources of variations in the mortality rates and to assess the risk factors contributing to mortality.
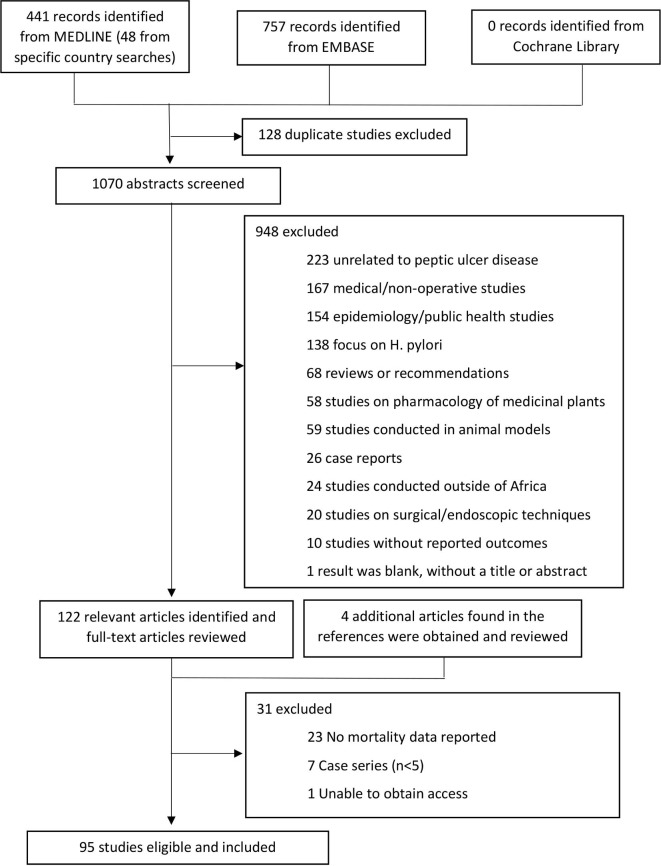
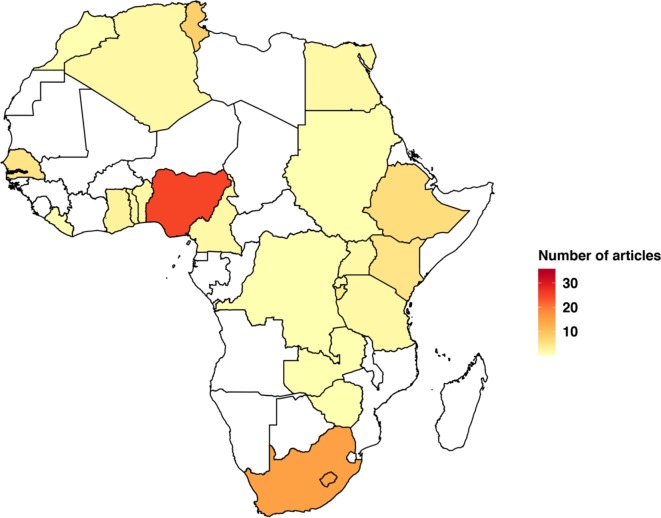
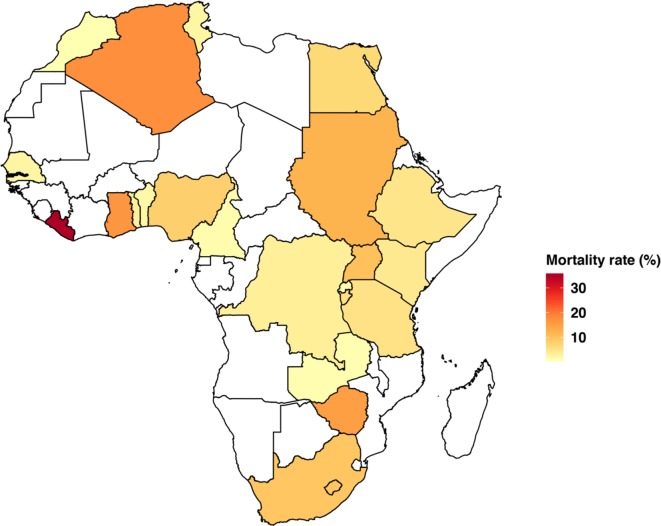
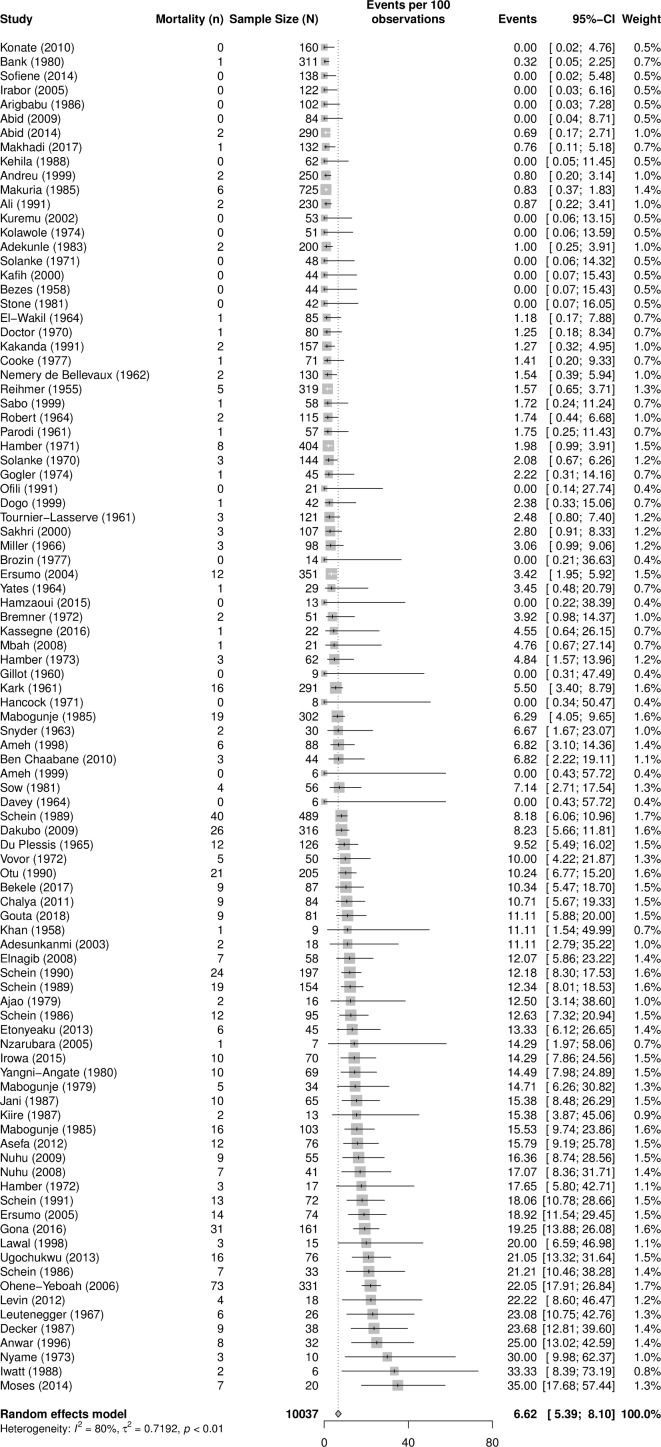
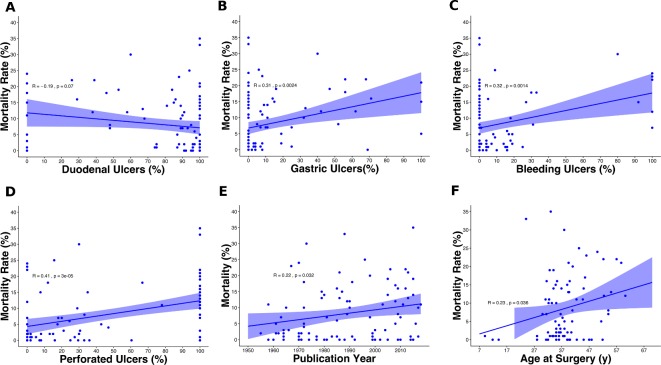
Results: From 95 published reports, 10 037 patients underwent surgery for complicated PUD. The majority of the ulcers (78%) were duodenal, followed by gastric (14%). Forty-one per cent of operations were for perforation, 22% for obstruction and 9% for bleeding. The operations consisted of vagotomy (38%), primary repair (34%), resection and reconstruction (12%), and drainage procedures (6%). The overall PUD mortality rate was 6.6% (95% CI 5.4% to 8.1%). It increased to 9.7% (95% CI 7.1 to 13.0) when we limited the analysis to studies published after the year 2000. The correlation was higher between perforated PUD and mortality rates (r=0.41, p<0.0001) than for bleeding PUD and mortality rates (r=0.32, p=0.001). Non-significant differences in mortality rates existed between sub-Saharan Africa (SSA) and North Africa and within SSA.
Conclusion: Perioperative mortality rates from complicated PUD in Africa are substantially high and could be increasing over time, and there are possible regional differences.
Keywords: Africa; bleeding; obstruction; peptic ulcer disease; perforation.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Surgery for Peptic Ulcer Disease in sub-Saharan Africa: Systematic Review of Published Data.J Gastrointest Surg. 2016 Apr;20(4):840-50. doi: 10.1007/s11605-015-3025-7. Epub 2015 Nov 16. J Gastrointest Surg. 2016. PMID: 26573850
-
The surgical management of complicated peptic ulcer disease: An EAST video presentation.J Trauma Acute Care Surg. 2022 Jul 1;93(1):e12-e16. doi: 10.1097/TA.0000000000003636. Epub 2022 Apr 1. J Trauma Acute Care Surg. 2022. PMID: 35358158 Free PMC article.
-
Short-term outcomes after emergency surgery for complicated peptic ulcer disease from the UK National Emergency Laparotomy Audit: a cohort study.BMJ Open. 2018 Aug 20;8(8):e023721. doi: 10.1136/bmjopen-2018-023721. BMJ Open. 2018. PMID: 30127054 Free PMC article.
-
Factors affecting mortality in patients operated upon for complications of peptic ulcer disease.Am Surg. 1989 Jan;55(1):7-11. Am Surg. 1989. PMID: 2913910
-
Prevalence and patterns of peptic ulcer disease in Africa: a systematic review and meta-analysis.BMC Gastroenterol. 2025 Apr 25;25(1):298. doi: 10.1186/s12876-025-03906-y. BMC Gastroenterol. 2025. PMID: 40281437 Free PMC article.
Cited by
-
Incidence of Acute Upper Gastrointestinal Bleeding and Related Risk Factors among Elderly Patients Undergoing Surgery for Major Limb Fractures: An Analytical Cohort Study.Healthcare (Basel). 2023 Oct 30;11(21):2853. doi: 10.3390/healthcare11212853. Healthcare (Basel). 2023. PMID: 37957997 Free PMC article.
-
Predictors of mortality for perforated peptic ulcer disease in Malawi.Am J Surg. 2023 Jun;225(6):1081-1085. doi: 10.1016/j.amjsurg.2022.11.029. Epub 2022 Nov 25. Am J Surg. 2023. PMID: 36481056 Free PMC article.
-
Non-steroidal Anti-inflammatory Drug (NSAID)-, Potassium Supplement-, Bisphosphonate-, and Doxycycline-Mediated Peptic Ulcer Effects: A Narrative Review.Cureus. 2024 Jan 8;16(1):e51894. doi: 10.7759/cureus.51894. eCollection 2024 Jan. Cureus. 2024. PMID: 38333496 Free PMC article. Review.
-
Upper gastrointestinal endoscopy findings in Mbale Regional Referral Hospital, Eastern Uganda: a 10-year retrospective analysis.Afr Health Sci. 2021 Jun;21(2):919-926. doi: 10.4314/ahs.v21i2.54. Afr Health Sci. 2021. PMID: 34795752 Free PMC article.
-
Unfavorable outcomes and their predictors in patients treated for perforated peptic ulcer disease in Ethiopia: systematic review and meta-analysis.BMC Gastroenterol. 2025 Apr 12;25(1):248. doi: 10.1186/s12876-025-03865-4. BMC Gastroenterol. 2025. PMID: 40221691 Free PMC article.
References
-
- Abubakar I, Tillmann T, GBD 2013 Mortality and Causes of Death Collaborators . Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the global burden of disease study 2013. Lancet 2015;385:117–71. 10.1016/S0140-6736(14)61682-2 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials