

Decision Tree-based Modelling for Identification of Predictors of Blood Loss and Transfusion Requirement After Adult Spinal Deformity Surgery
- PMID: 32128308
- PMCID: PMC7043811
- DOI: 10.14444/7012
Decision Tree-based Modelling for Identification of Predictors of Blood Loss and Transfusion Requirement After Adult Spinal Deformity Surgery
Abstract
Background: Multilevel fusions and complex osteotomies to restore global alignment in adult spinal deformity (ASD) surgery can lead to increased operative time and blood loss. In this regard, we assessed factors predictive of perioperative blood product transfusion in patients undergoing long posterior spinal fusion for ASD.
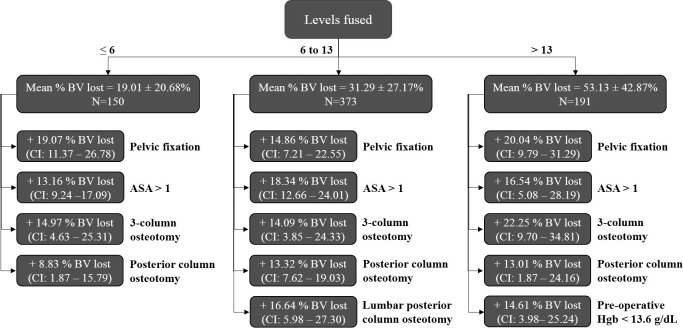
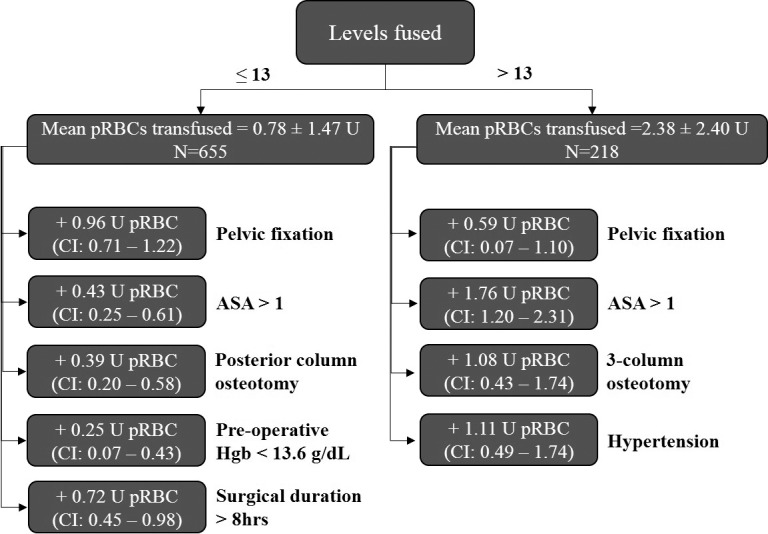
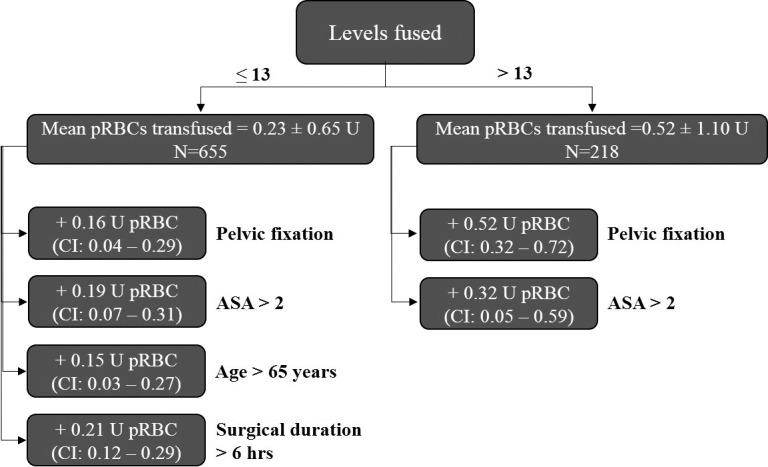
Methods: A single-institution retrospective review was conducted on 909 patients with ASD, age > 18 years, who underwent surgery for ASD with greater than 4 levels fused. Using conditional inference tree analysis, a machine learning methodology, we sought to predict the combination of variables that best predicted increased risk for intraoperative percent blood volume lost and perioperative blood product transfusion.
Results: Among the 909 patients included in the study, 377 (41.5%) received red blood cell (RBC) transfusion. The conditional inference tree analysis identified greater than 13 levels fused, American Society of Anesthesiologists (ASA) score > 1, a history of hypertension, 3-column osteotomy, pelvic fixation, and operative time > 8 hours, as significant risk factors for perioperative RBC transfusion. The best predictors for the subgroup with the highest risk for intraoperative percent blood volume lost (subgroup mean: 53.1% ± 42.9%) were greater than 13 levels fused, ASA score > 1, preoperative hemoglobin < 13.6 g/dL, 3-column osteotomy, posterior column osteotomy, and pelvic fixation. Patients who underwent major blood transfusion intraoperatively had significantly longer length of stay (8.5 days) versus those who did not (6.1 days) (P < .0001). The overall 90-day complication rate in patients who underwent major blood transfusion intraoperatively was 49%, compared with 19% in those who did not (P < .0001). By multivariate regression analysis, patients with a preoperative hemoglobin > 13.0 were less likely to require major blood transfusion (odds ratio: 0.52, P = .046).
Conclusions: Using a supervised learning technique, this study demonstrates that greater than 13 levels fused, ASA score > 1, 3-column osteotomy, and pelvic fixation are consistent risk factors for increased intraoperative percent blood volume lost and perioperative RBC transfusion. The addition of having a preoperative hemoglobin < 13.6 g/dL or undergoing a posterior column osteotomy conferred the highest risk for intraoperative blood loss. This information can assist spinal deformity surgeons in identifying at-risk individuals and allocating healthcare resources.
Level of evidence: 3.
Keywords: blood product transfusion; complex spine surgery; perioperative blood loss.
©International Society for the Advancement of Spine Surgery 2020.
Conflict of interest statement
Disclosures and COI: The authors received no funding for this study and report no conflicts of interest.
Figures
Similar articles
-
Risk factors for allogeneic red blood cell transfusion in adult spinal deformity surgery.Asian Spine J. 2024 Aug;18(4):579-586. doi: 10.31616/asj.2024.0080. Epub 2024 Aug 20. Asian Spine J. 2024. PMID: 39164025 Free PMC article.
-
Determinants of perioperative transfusion risk in patients with adult spinal deformity.J Neurosurg Spine. 2018 Apr;28(4):429-435. doi: 10.3171/2017.10.SPINE17884. Epub 2018 Jan 19. J Neurosurg Spine. 2018. PMID: 29350594
-
Rotational thromboelastometry-guided transfusion during lumbar pedicle subtraction osteotomy for adult spinal deformity: preliminary findings from a matched cohort study.Neurosurg Focus. 2019 Apr 1;46(4):E17. doi: 10.3171/2019.1.FOCUS18572. Neurosurg Focus. 2019. PMID: 30933918
-
Risk Factors for Perioperative Blood Transfusions in Adult Spinal Deformity Surgery.World Neurosurg. 2018 Jul;115:e731-e737. doi: 10.1016/j.wneu.2018.04.152. Epub 2018 Apr 30. World Neurosurg. 2018. PMID: 29715572
-
Safe and effective performance of pediatric spinal deformity surgery in patients unwilling to accept blood transfusion: a clinical study and review of literature.BMC Musculoskelet Disord. 2021 Feb 19;22(1):204. doi: 10.1186/s12891-021-04081-3. BMC Musculoskelet Disord. 2021. PMID: 33607982 Free PMC article. Review.
Cited by
-
AI and machine learning in paediatric spine deformity surgery.Bone Jt Open. 2025 May 23;6(5):569-581. doi: 10.1302/2633-1462.65.BJO-2024-0089.R1. Bone Jt Open. 2025. PMID: 40407025 Free PMC article.
-
Machine learning in transfusion medicine: A scoping review.Transfusion. 2024 Jan;64(1):162-184. doi: 10.1111/trf.17582. Epub 2023 Nov 10. Transfusion. 2024. PMID: 37950535 Free PMC article. No abstract available.
-
Emerging Technologies in the Treatment of Adult Spinal Deformity.Neurospine. 2021 Sep;18(3):417-427. doi: 10.14245/ns.2142412.206. Epub 2021 Sep 30. Neurospine. 2021. PMID: 34610669 Free PMC article.
-
Assessing blood volume returned with use of intraoperative cell salvage in adult spinal deformity correction.Spine Deform. 2025 Jul;13(4):1223-1229. doi: 10.1007/s43390-025-01055-6. Epub 2025 Feb 17. Spine Deform. 2025. PMID: 39962009
-
Risk factors for allogeneic red blood cell transfusion in adult spinal deformity surgery.Asian Spine J. 2024 Aug;18(4):579-586. doi: 10.31616/asj.2024.0080. Epub 2024 Aug 20. Asian Spine J. 2024. PMID: 39164025 Free PMC article.
References
-
- Cha CW, Deible C, Muzzonigro T, Lopez-Plaza I, Vogt M, Kang JD. Allogeneic transfusion requirements after autologous donations in posterior lumbar surgeries. Spine. 2002;27(1):99–104. - PubMed
-
- Johnson RG, Murphy M, Miller M. Fusions and transfusions. An analysis of blood loss and autologous replacement during lumbar fusions. Spine. 1989;14(4):358–362. - PubMed
-
- Guay J, Haig M, Lortie L, Guertin MC, Poitras B. Predicting blood loss in surgery for idiopathic scoliosis. Can J Anaesth. 1994;41(9):775–781. - PubMed
-
- Zheng F, Cammisa FP, Jr, Sandhu HS, Girardi FP, Khan SN. Factors predicting hospital stay, operative time, blood loss, and transfusion in patients undergoing revision posterior lumbar spine decompression, fusion, and segmental instrumentation. Spine. 2002;27(8):818–824. - PubMed
-
- Cassinelli EH, Eubanks J, Vogt M, Furey C, Yoo J, Bohlman HH. Risk factors for the development of perioperative complications in elderly patients undergoing lumbar decompression and arthrodesis for spinal stenosis: an analysis of 166 patients. Spine. 2007;32:230–235. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials