

Adenotonsillectomy and postoperative respiratory adverse events: A retrospective study
- PMID: 32128445
- PMCID: PMC7042638
- DOI: 10.1002/lio2.340
Adenotonsillectomy and postoperative respiratory adverse events: A retrospective study
Abstract
Objectives: Postoperative respiratory adverse events (PRAEs) are known complications following adenotonsillectomy (AT). Clinical data at a single institution were reviewed to investigate the factors that may contribute to PRAEs in the postanesthesia care unit (PACU). The relationship between PRAEs in the PACU and escalation of care, defined as either an unplanned admission for outpatient surgery or unplanned pediatric intensive care unit (PICU) admission, was investigated.
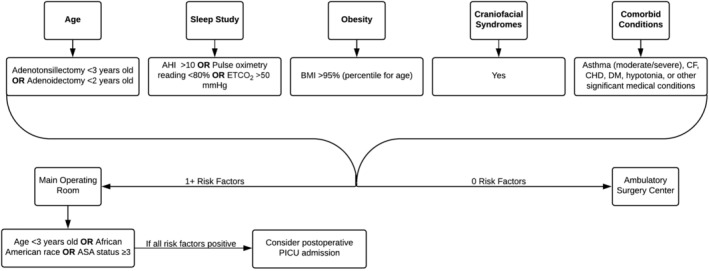
Methods: The perioperative records for all patients who underwent AT from 2016 to 2018 were reviewed. The surgical procedure was performed at both the main campus and the ambulatory surgery center in accordance with the institutional obstructive sleep apnea (OSA) guidelines. Patient characteristics and intraoperative medications were compared. Categorical variables were summarized as counts with percentages and compared using chi-square tests or Fisher's exact tests. Continuous variables were summarized as medians with interquartile ranges and compared using rank-sum tests. Multivariable logistic regression was performed to evaluate the association of intraoperative dosing with the occurrence of PRAEs.
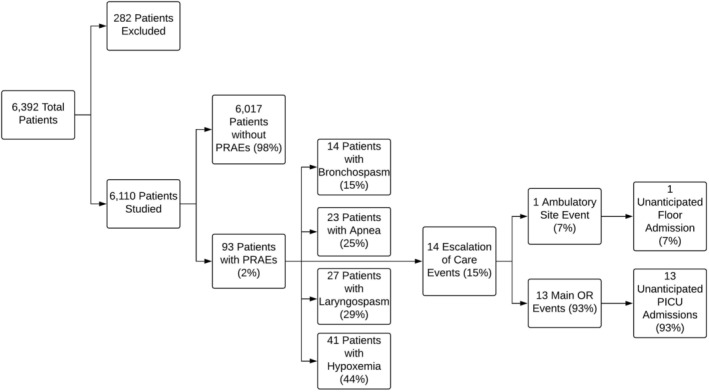
Results: The study cohort included 6110 patients. Ninety-three patients (2%) experienced PRAEs in the PACU. Of these 93 patients, 14 (15%) resulted in an escalation of care, nearly all of which were unplanned PICU admissions. PRAEs tended to occur in younger patients, non-Hispanic black patients, and those with a higher American Society of Anesthesiologists (ASA) status.
Conclusions: PRAEs are infrequent after AT at a tertiary institution with OSA guidelines in place. However, when PRAEs do occur, escalation of care may be required. Risk factors include age, ethnic background, and ASA physical status.
Level of evidence: III.
Keywords: adenotonsillectomy; hypoxemia; laryngospasm; respiratory; tonsillectomy.
© 2019 The Authors. Laryngoscope Investigative Otolaryngology published by Wiley Periodicals, Inc. on behalf of The Triological Society.
Conflict of interest statement
T.B.H., A.T., J.D.T., and V.T.R. declare no potential conflict of interest. K.R.J. receives royalties from Marpac, Inc. for a patented tracheostomy collar design, commercially available, and from a product safety medical consultant, Intertek, Inc.
Figures
References
-
- Cohen N, Sommer DD. Post‐tonsillectomy pain control: consensus or controversy? Pain Manage. 2016;6:31‐37. - PubMed
-
- Nixon GM, Kermack AS, Mcgregor CD, et al. Sleep and breathing on the first night after adenotonsillectomy for obstructive sleep apnea. Pediatr Pulm. 2005;39(4):332‐338. - PubMed
-
- Arambula AM, Xie DX, Whigham AS. Respiratory events after adenotonsillectomy requiring escalated admission status in children with obstructive sleep apnea. Int J Pediatr Otorhinol. 2018;107:31‐36. - PubMed
-
- Subramanyam R, Yeramaneni S, Hossain MM, Anneken AM, Varughese AM. Perioperative respiratory adverse events in pediatric ambulatory anesthesia. Anesth Analg. 2016;122:1578‐1585. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Research Materials