Metabolically Healthy Obesity
- PMID: 32128581
- PMCID: PMC7098708
- DOI: 10.1210/endrev/bnaa004
Metabolically Healthy Obesity
Abstract
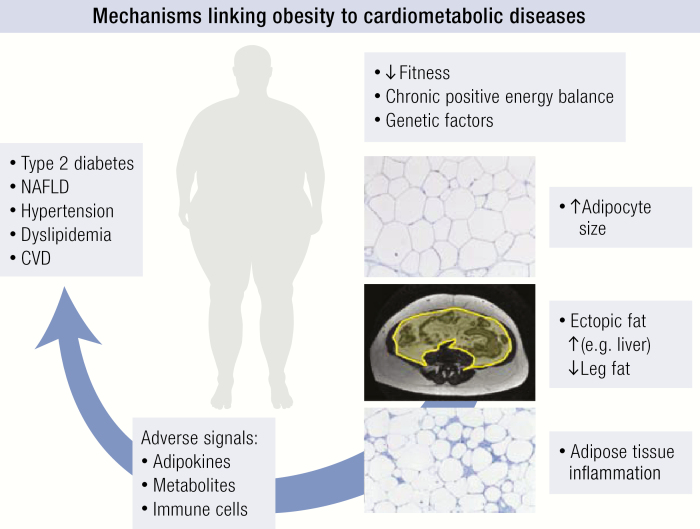
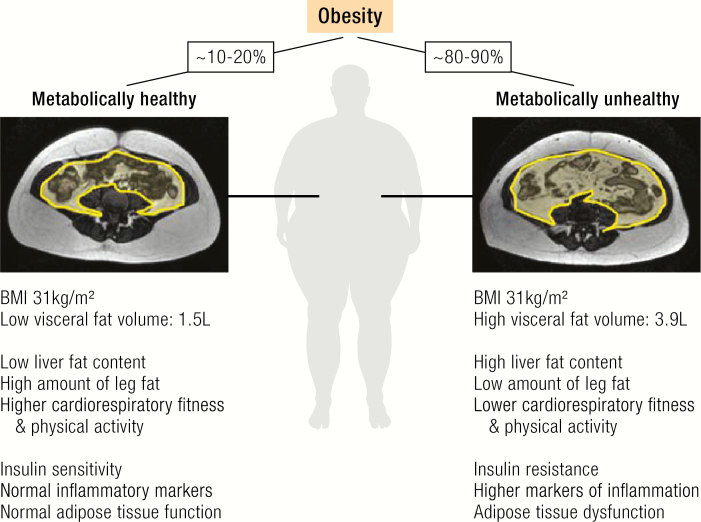
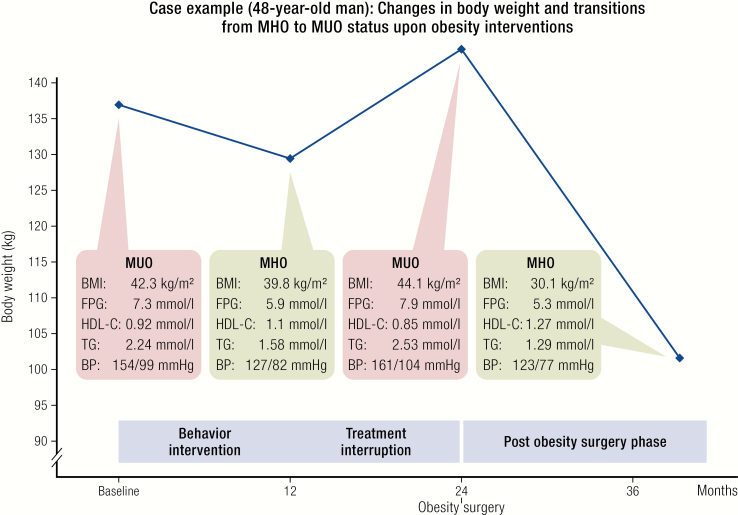
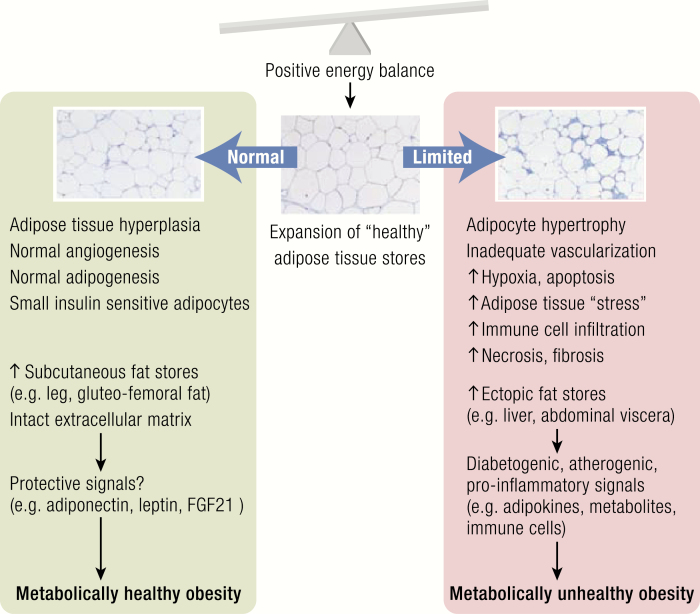
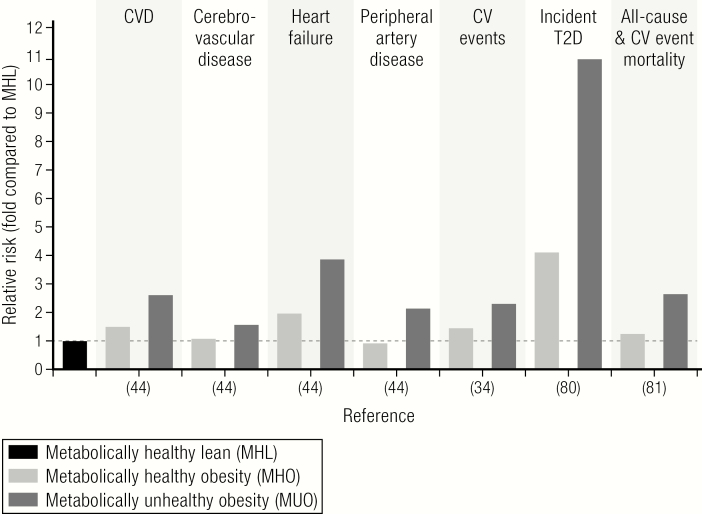
Obesity contributes to reduced life expectancy, impaired quality of life, and disabilities, mainly in those individuals who develop cardiovascular diseases, type 2 diabetes, osteoarthritis, and cancer. However, there is a large variation in the individual risk to developing obesity-associated comorbid diseases that cannot simply be explained by the extent of adiposity. Observations that a proportion of individuals with obesity have a significantly lower risk for cardiometabolic abnormalities led to the concept of metabolically healthy obesity (MHO). Although there is no clear definition, normal glucose and lipid metabolism parameters-in addition to the absence of hypertension-usually serve as criteria to diagnose MHO. Biological mechanisms underlying MHO lower amounts of ectopic fat (visceral and liver), and higher leg fat deposition, expandability of subcutaneous adipose tissue, preserved insulin sensitivity, and beta-cell function as well as better cardiorespiratory fitness compared to unhealthy obesity. Whereas the absence of metabolic abnormalities may reduce the risk of type 2 diabetes and cardiovascular diseases in metabolically healthy individuals compared to unhealthy individuals with obesity, it is still higher in comparison with healthy lean individuals. In addition, MHO seems to be a transient phenotype further justifying therapeutic weight loss attempts-even in this subgroup-which might not benefit from reducing body weight to the same extent as patients with unhealthy obesity. Metabolically healthy obesity represents a model to study mechanisms linking obesity to cardiometabolic complications. Metabolically healthy obesity should not be considered a safe condition, which does not require obesity treatment, but may guide decision-making for a personalized and risk-stratified obesity treatment.
© Endocrine Society 2020.
Figures