

Prospective assessment of loss to follow-up: incidence and associated factors in a cohort of HIV-positive adults in rural Tanzania
- PMID: 32128998
- PMCID: PMC7054631
- DOI: 10.1002/jia2.25460
Prospective assessment of loss to follow-up: incidence and associated factors in a cohort of HIV-positive adults in rural Tanzania
Abstract
Introduction: Lifelong antiretroviral therapy (ART) improves health outcomes for HIV-positive individuals, but is jeopardized by irregular clinic attendance and hence poor adherence. Loss to follow-up (LTFU) is typically defined retrospectively but this may lead to biased inferences. We assessed incidence of and factors associated with LTFU, prospectively and accounting for recurrent LTFU episodes, in the Kilombero and Ulanga Antiretroviral Cohort (KIULARCO) of HIV-positive persons in rural Tanzania.
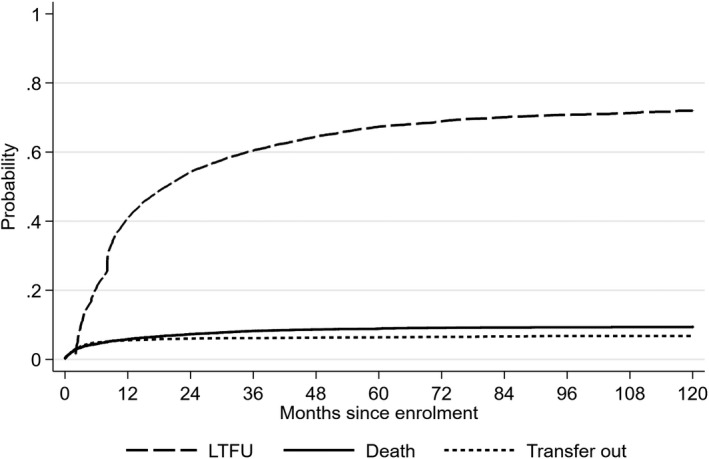
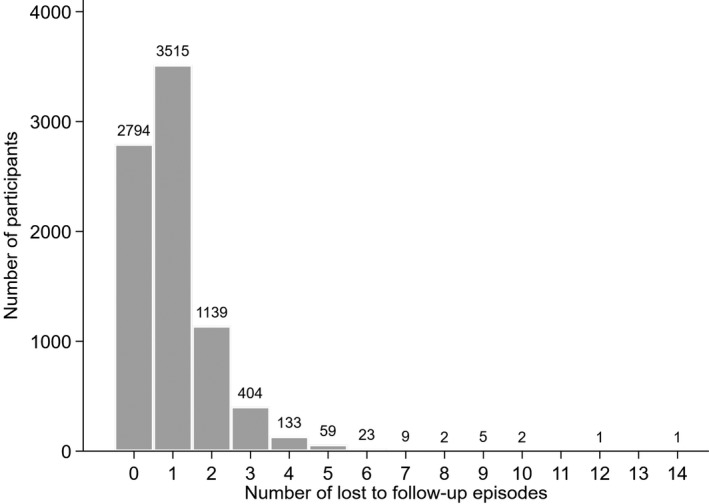
Methods: We included adults (≥15 years) enrolled in 2005 to 2016, regardless of ART status, with follow-up through April 2017. LTFU was defined as >60 days late for a scheduled appointment. Participants could experience multiple LTFU episodes. We performed analyses based on the first (prospective) and last (retrospective) events observed during follow-up, and accounting for recurrent LTFU episodes. Time to LTFU was estimated using cumulative incidence functions. We assessed factors associated with LTFU using cause-specific proportional hazards, marginal means/rates, and Prentice, Williams and Peterson models.
Results: Among 8087 participants (65% female, 60% aged ≥35 years, 42% WHO stage 3/4, and 47% CD4 count <200 cells/mm3 ), there were 8140 LTFU episodes, after which there were 2483 (31%) returns to care. One-year LTFU probabilities were 0.41 (95% confidence interval 0.40, 0.42) and 0.21 (0.20, 0.22) considering the first and last events respectively. Factors associated with LTFU were broadly consistent across different models: being male, younger age, never married, living far from the clinic, not having an HIV-positive partner, lower BMI, advanced WHO stage, not having tuberculosis, and shorter time since ART initiation. Associations between LTFU and pregnancy, CD4 count, and enrolment year depended on the analysis approach.
Conclusions: LTFU episodes were common and prompt tracing efforts are urgently needed. We identified socio-demographic and clinical characteristics associated with LTFU that can be used to target tracing efforts and to help inform the design of appropriate interventions. Incidence of and risk factors for LTFU differed based on the LTFU definition applied, highlighting the importance of appropriately accounting for recurrent LTFU episodes. We recommend using a prospective definition of LTFU combined with recurrent event analyses in cohorts where repeated interruptions in care are common.
Keywords: HIV infections; Tanzania; cohort; lost to follow-up; proportional hazards models; recurrent events.
© 2020 The Authors. Journal of the International AIDS Society published by John Wiley & Sons Ltd on behalf of the International AIDS Society.
Figures
References
-
- UNAIDS . 90–90‐90 An ambitious treatment target to help end the AIDS epidemic. Geneva, Switzerland: UNAIDS; 2014.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
