

Male and Female Physician Suicidality: A Systematic Review and Meta-analysis
- PMID: 32129813
- PMCID: PMC7057173
- DOI: 10.1001/jamapsychiatry.2020.0011
Male and Female Physician Suicidality: A Systematic Review and Meta-analysis
Abstract
Importance: Population-based findings on physician suicide are of great relevance because this is an important and understudied topic.
Objective: To evaluate male and female physician suicide risks compared with the general population from 1980 to date and test whether there is a reduction of SMR in cohorts after 1980 compared with before 1980 via a meta-analysis, modeling studies, and a systematic review emphasizing physician suicide risk factors.
Data sources: This study uses studies retrieved from PubMed, Scielo, PsycINFO, and Lilacs for human studies published by October 3, 2019, using the search term "(((suicide) OR (self-harm) OR (suicidality)) AND ((physicians) OR (doctors)))." Databases were also searched from countries listed in articles selected for review. Data were also extracted from an existing article by other authors to facilitate comparisons of the pre-1980 suicide rate with the post-1980 changes.
Study selection: Original articles assessing male and/or female physician suicide were included; for the meta-analysis, only cohorts from 1980 to the present were included.
Data extraction and synthesis: The preregistered systematic review and meta-analysis followed Cochrane, PRISMA, and MOOSE guidelines. Data were extracted into standardized tables per a prespecified structured checklist, and quality scores were added. Heterogeneity was tested via Q test, I2, and τ2. For pooled effect estimates, we used random-effects models. The Begg and Egger tests, sensitivity analyses, and meta-regression were performed. Proportional mortality ratios were presented when SMR data could not be extracted.
Main outcomes and measures: Suicide SMRs for male and female physicians from 1980 to the present and changes over time (before and after 1980).
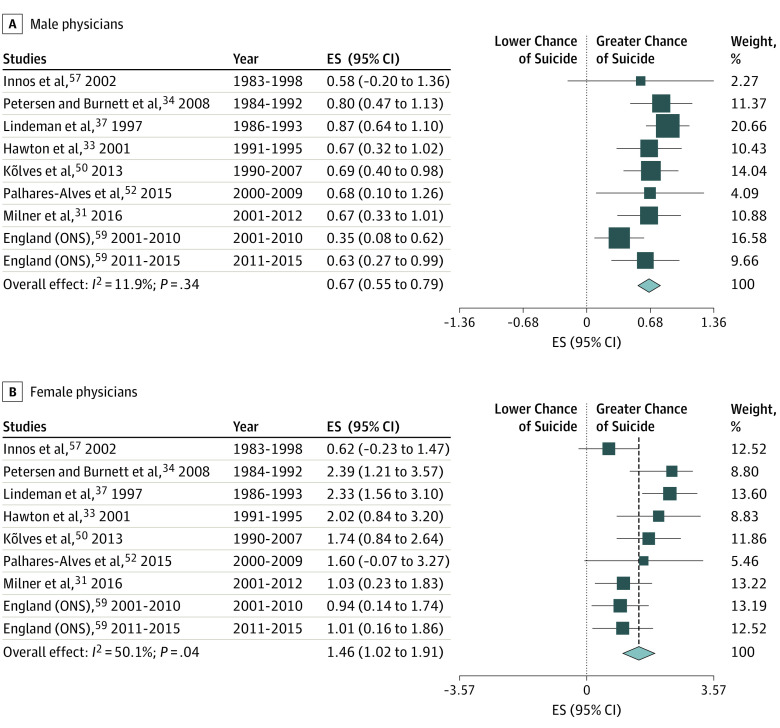
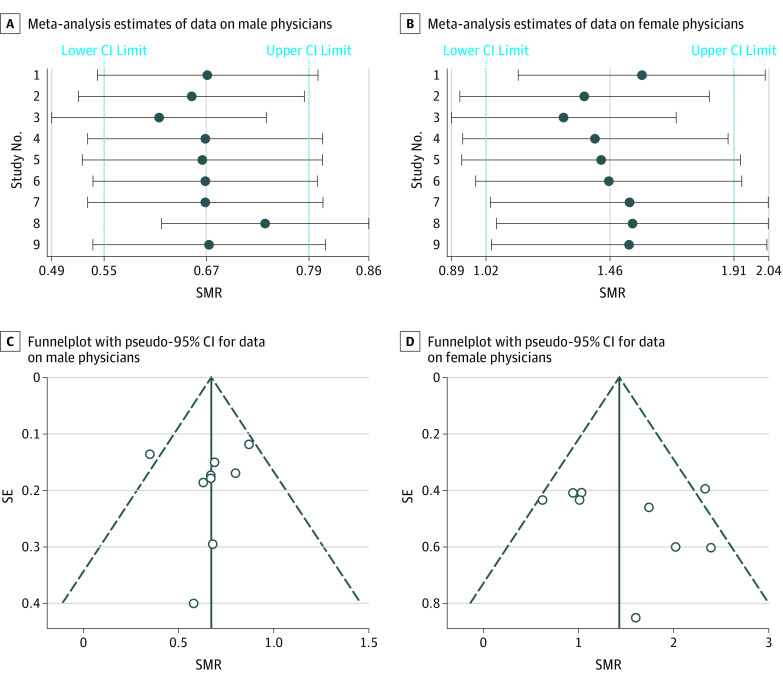
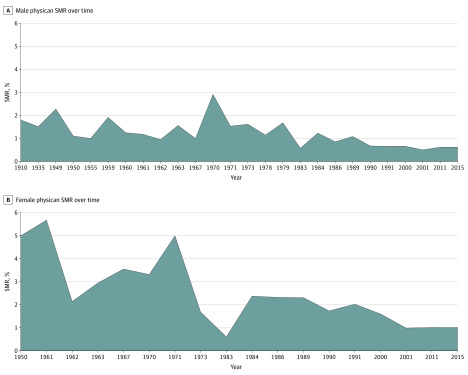
Results: Of 7877 search results, 32 articles were included in the systematic review and 9 articles and data sets in the meta-analysis. Meta-analysis showed a significantly higher suicide SMR in female physicians compared with women in general (1.46 [95% CI, 1.02-1.91]) and a significantly lower suicide SMR in male physicians compared with men in general (0.67 [95% CI, 0.55-0.79]). Male and female physician SMRs significantly decreased after 1980 vs before 1980 (male physicians: SMR, -0.84 [95% CI, -1.26 to -0.42]; P < .001; female physicians: SMR, -1.96 [95% CI, -3.09 to -0.84]; P = .002). No evidence of publication bias was found.
Conclusions and relevance: In this study, suicide SMR was found to be high in female physicians and low in male physicians since 1980 but also to have decreased over time in both groups. Physician suicides are multifactorial, and further research into these factors is critical.
Conflict of interest statement
Figures
Comment in
-
Physician Suicide-A Personal and Community Tragedy.JAMA Psychiatry. 2020 Jun 1;77(6):559-560. doi: 10.1001/jamapsychiatry.2020.0009. JAMA Psychiatry. 2020. PMID: 32129812 No abstract available.
References
-
- World Health Organization Suicide data. https://www.who.int/mental_health/prevention/suicide/suicideprevent/en/#.... Published 2018. Accessed January 15, 2020.
-
- World Health Organization Disease burden and mortality estimates. https://www.who.int/healthinfo/global_burden_disease/estimates/en/index1.... Published 2019. Accessed January 15, 2020.
-
- Wang H, Naghavi M, Allen C, et al. ; GBD 2015 Mortality and Causes of Death Collaborators . Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1459-1544. doi:10.1016/S0140-6736(16)31012-1 - DOI - PMC - PubMed
-
- Ivey-Stephenson AZ, Crosby AE, Jack SPD, Haileyesus T, Kresnow-Sedacca M-J. Suicide trends among and within urbanization levels by sex, race/ethnicity, age group, and mechanism of death—United States, 2001-2015. MMWR Surveill Summ. 2017;66(18):1-16. https://www.ncbi.nlm.nih.gov/pubmed/28981481. Internet. doi:10.15585/mmwr.ss6618a1 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
