

Remote Management of Poststroke Patients With a Smartphone-Based Management System Integrated in Clinical Care: Prospective, Nonrandomized, Interventional Study
- PMID: 32130140
- PMCID: PMC7068458
- DOI: 10.2196/15377
Remote Management of Poststroke Patients With a Smartphone-Based Management System Integrated in Clinical Care: Prospective, Nonrandomized, Interventional Study
Abstract
Background: Advances in mobile health (mHealth) have enabled systematic and continuous management of patients with chronic diseases.
Objective: We developed a smartphone-based mHealth system and aimed to evaluate its effects on health behavior management and risk factor control in stroke patients.
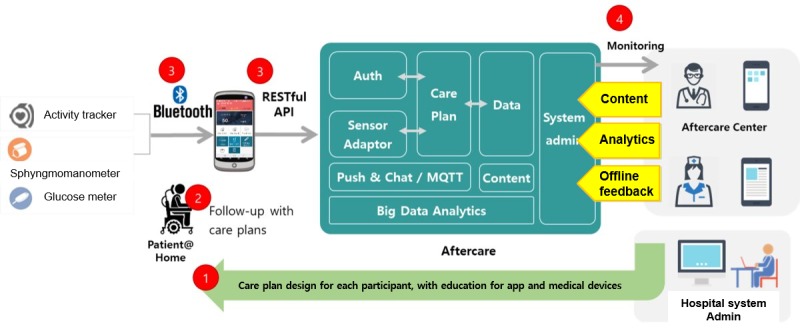
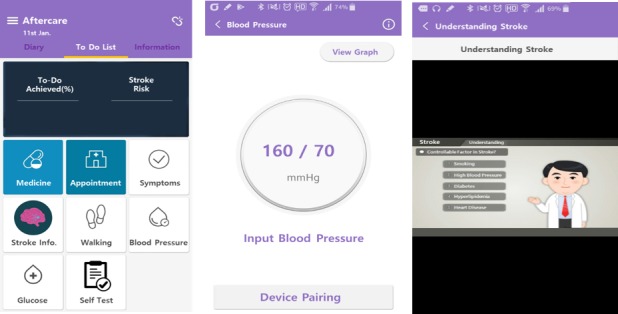
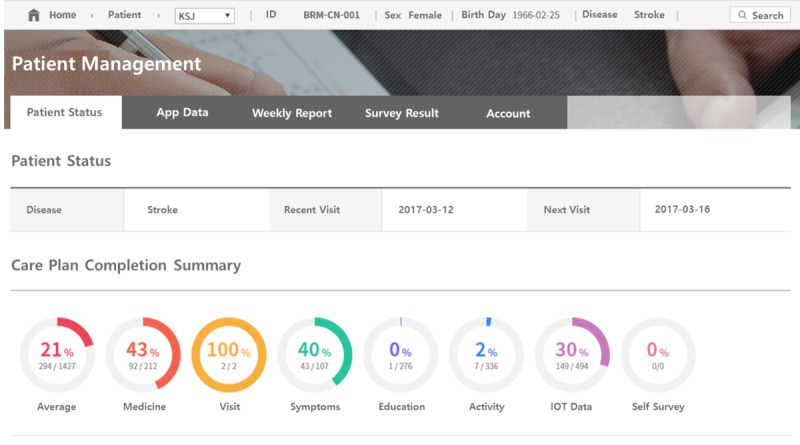
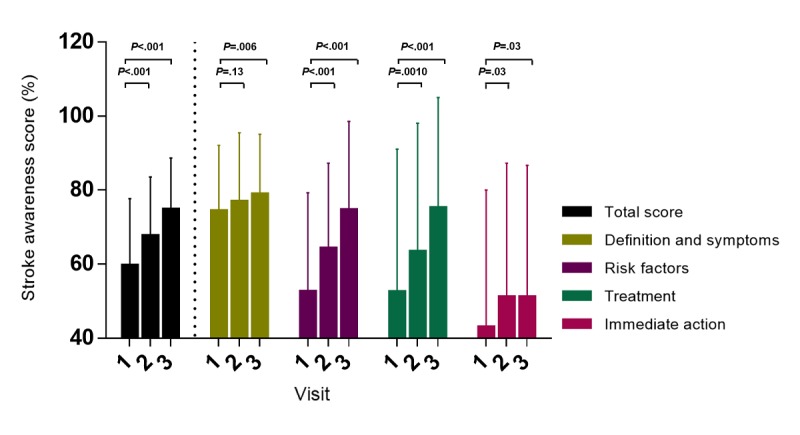
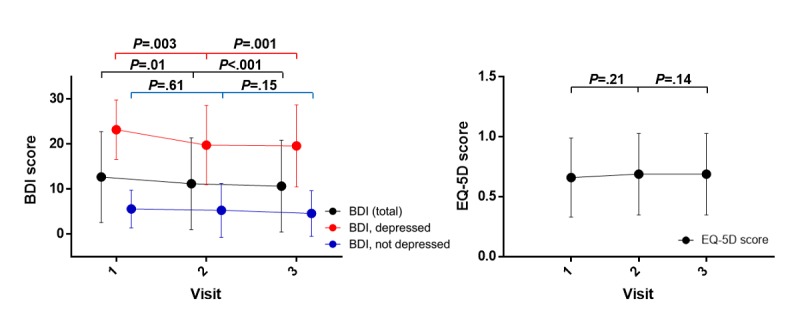
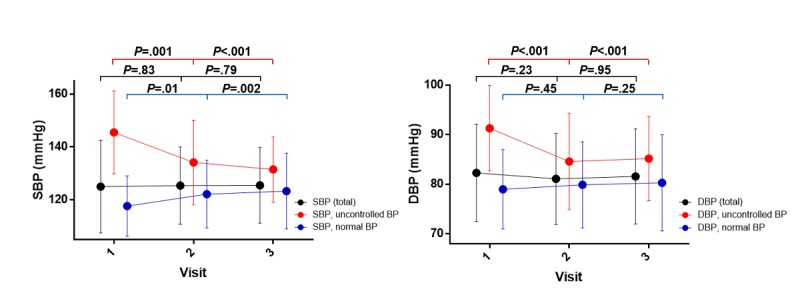
Methods: With a multifaceted stroke aftercare management system that included exercise, medication, and educational materials, we performed a 12-week single-arm intervention among eligible poststroke patients in the stroke clinic from September to December 2016. The intervention consisted of (1) regular blood pressure (BP), blood glucose, and physical activity measurements; (2) stroke education; (3) an exercise program; (4) a medication program; and (5) feedback on reviewing of records by clinicians. Clinical assessments consisted of the stroke awareness score, Beck Depression Inventory-II (BDI), EuroQol-5 Dimensions (EQ-5D), and BP at visit 1 (baseline), visit 2 (4 weeks), and visit 3 (12 weeks). Temporal differences in the parameters over 12 weeks were investigated with repeated-measures analysis of variance. Changes in medication adherence at visit 1-2 (from visit 1 to visit 2) and visit 2-3 (from visit 2 to visit 3) were compared. System satisfaction was evaluated with a self-questionnaire using a 5-point Likert scale at visit 3.
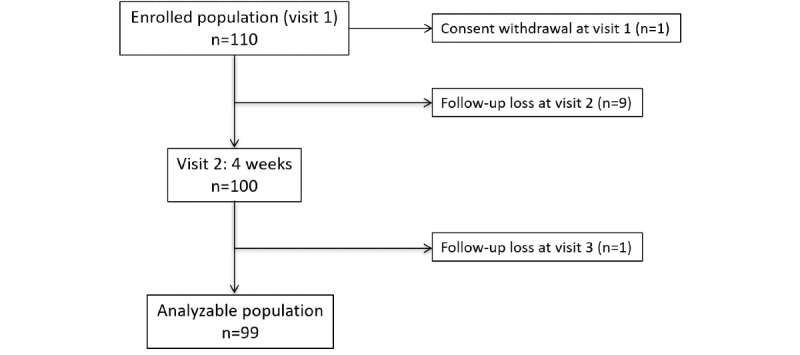
Results: The study was approved by the Institutional Review Board in September 2016, and participants were enrolled from September to December 2016. Among the 110 patients enrolled for the study, 99 were included in our analyses. The mean stroke awareness score (baseline: 59.6 [SD 18.1]; 4 weeks: 67.6 [SD 16.0], P<.001; 12 weeks: 74.7 [SD 14.0], P<.001) and BDI score (baseline: 12.7 [SD 10.1]; 4 weeks: 11.2 [SD 10.2], P=.01; 12 weeks: 10.7 [SD 10.2], P<.001) showed gradual improvement; however, no significant differences were found in the mean EQ-5D score (baseline: 0.66 [SD 0.33]; 4 weeks: 0.69 [SD 0.34], P=.01; 12 weeks: 0.69 [SD 0.34], P<.001). Twenty-six patients who had uncontrolled BP at baseline had -13.92 mmHg (P=.001) and -6.19 mmHg (P<.001) reductions on average in systolic and diastolic BP, respectively, without any antihypertensive medication change. Medication compliance was better at visit 2-3 (60.9% [SD 37.2%]) than at visit 1-2 (47.8% [SD 38.7%], P<.001).
Conclusions: Awareness of stroke, depression, and BP was enhanced when using the smartphone-based mHealth system. Emerging mHealth techniques have potential as new nonpharmacological secondary prevention methods because of their ubiquitous access, near real-time responsiveness, and comparatively lower cost.
Keywords: health care; mHealth; mobile apps; patient education; self-monitoring of blood pressure; stroke care.
©Do Yeon Kim, Hee Kwon, Ki-Woong Nam, Yongseok Lee, Hyung-Min Kwon, Young Seob Chung. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 27.02.2020.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Hardie K, Hankey GJ, Jamrozik K, Broadhurst RJ, Anderson C. Ten-year survival after first-ever stroke in the perth community stroke study. Stroke. 2003 Aug;34(8):1842–6. doi: 10.1161/01.STR.0000082382.42061.EE. - DOI - PubMed
-
- Luengo-Fernandez R, Gray AM, Rothwell PM, Oxford Vascular Study A population-based study of hospital care costs during 5 years after transient ischemic attack and stroke. Stroke. 2012 Dec;43(12):3343–51. doi: 10.1161/STROKEAHA.112.667204. http://europepmc.org/abstract/MED/23160884 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
