

Analyzing Medical Research Results Based on Synthetic Data and Their Relation to Real Data Results: Systematic Comparison From Five Observational Studies
- PMID: 32130148
- PMCID: PMC7059086
- DOI: 10.2196/16492
Analyzing Medical Research Results Based on Synthetic Data and Their Relation to Real Data Results: Systematic Comparison From Five Observational Studies
Abstract
Background: Privacy restrictions limit access to protected patient-derived health information for research purposes. Consequently, data anonymization is required to allow researchers data access for initial analysis before granting institutional review board approval. A system installed and activated at our institution enables synthetic data generation that mimics data from real electronic medical records, wherein only fictitious patients are listed.
Objective: This paper aimed to validate the results obtained when analyzing synthetic structured data for medical research. A comprehensive validation process concerning meaningful clinical questions and various types of data was conducted to assess the accuracy and precision of statistical estimates derived from synthetic patient data.
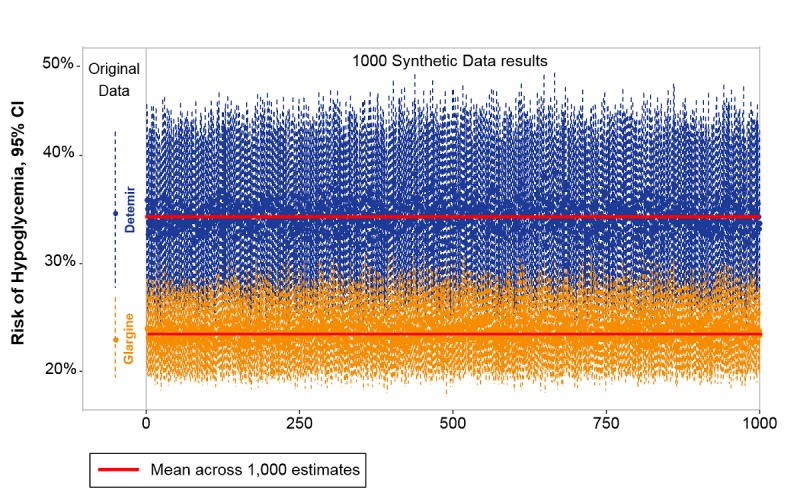
Methods: A cross-hospital project was conducted to validate results obtained from synthetic data produced for five contemporary studies on various topics. For each study, results derived from synthetic data were compared with those based on real data. In addition, repeatedly generated synthetic datasets were used to estimate the bias and stability of results obtained from synthetic data.
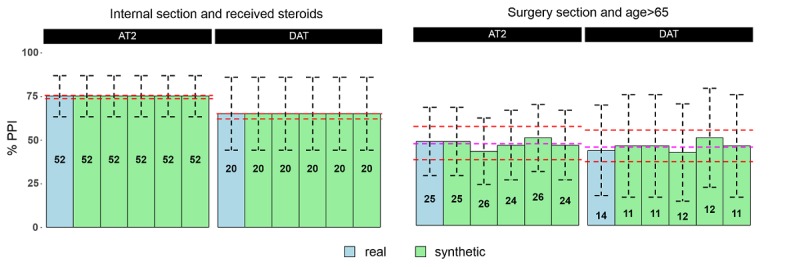
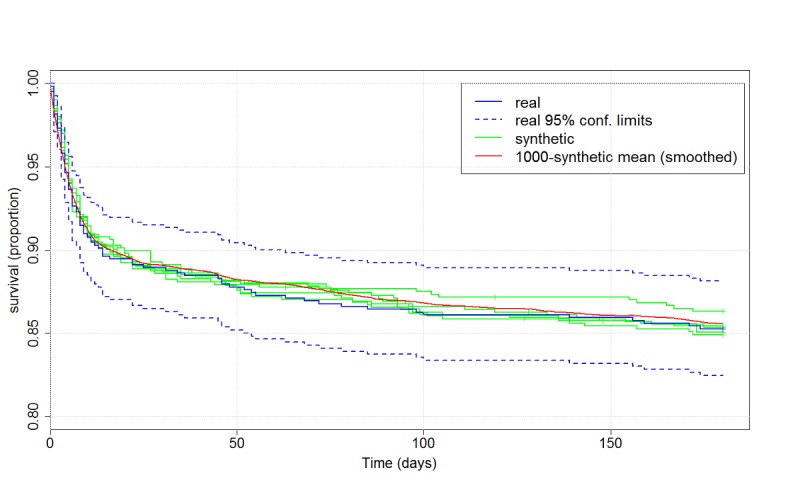
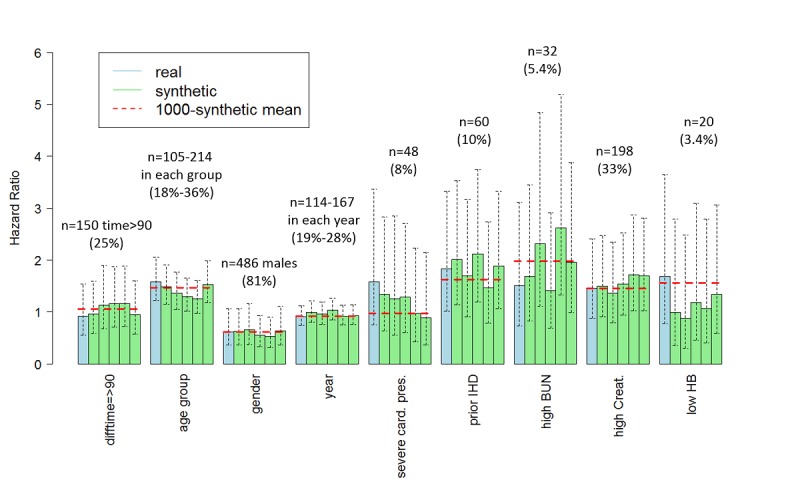
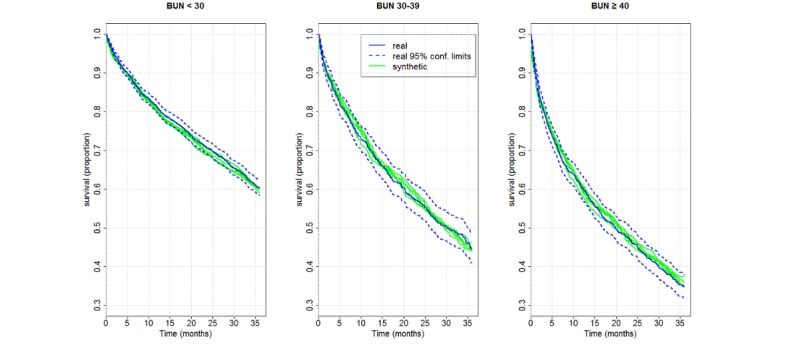
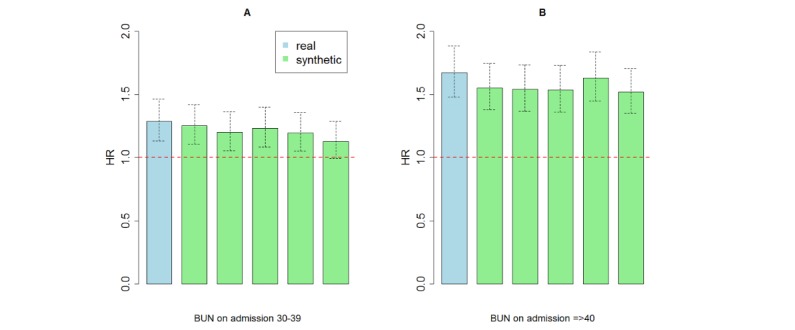
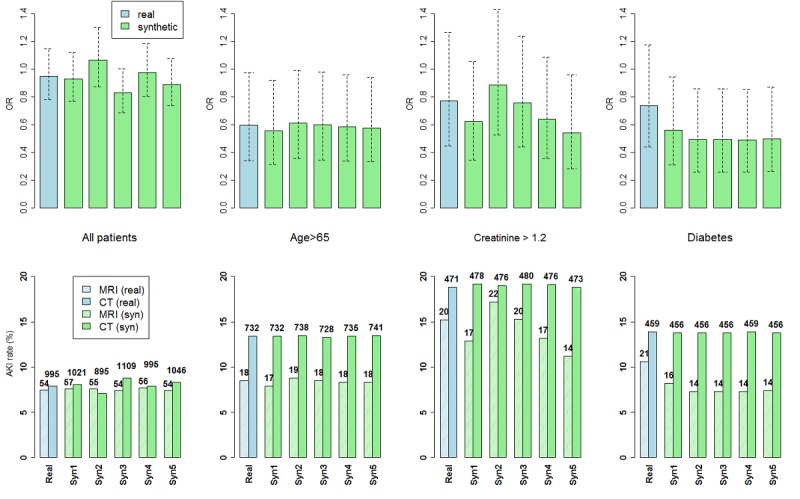
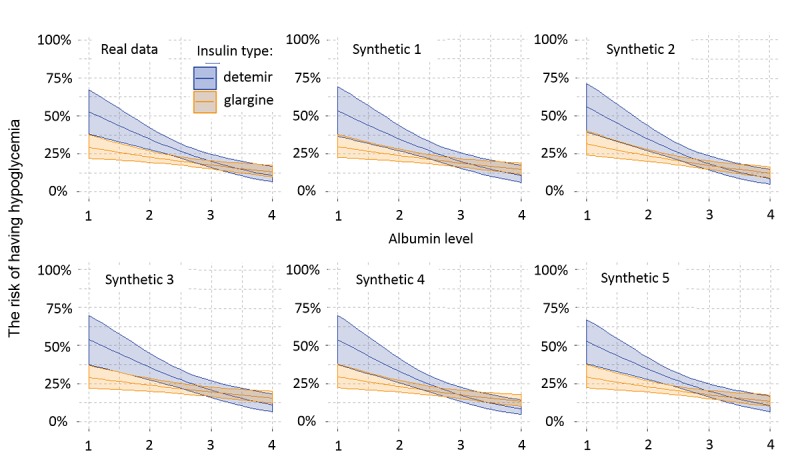
Results: This study demonstrated that results derived from synthetic data were predictive of results from real data. When the number of patients was large relative to the number of variables used, highly accurate and strongly consistent results were observed between synthetic and real data. For studies based on smaller populations that accounted for confounders and modifiers by multivariate models, predictions were of moderate accuracy, yet clear trends were correctly observed.
Conclusions: The use of synthetic structured data provides a close estimate to real data results and is thus a powerful tool in shaping research hypotheses and accessing estimated analyses, without risking patient privacy. Synthetic data enable broad access to data (eg, for out-of-organization researchers), and rapid, safe, and repeatable analysis of data in hospitals or other health organizations where patient privacy is a primary value.
Keywords: MDClone; big data analysis; electronic medical records; synthetic data; validation study.
©Anat Reiner Benaim, Ronit Almog, Yuri Gorelik, Irit Hochberg, Laila Nassar, Tanya Mashiach, Mogher Khamaisi, Yael Lurie, Zaher S Azzam, Johad Khoury, Daniel Kurnik, Rafael Beyar. Originally published in JMIR Medical Informatics (http://medinform.jmir.org), 20.02.2020.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Garfinkle SL. National Institute of Standards and Technology. 2015. Oct, [2020-01-20]. De-Identification of Personal Information https://nvlpubs.nist.gov/nistpubs/ir/2015/NIST.IR.8053.pdf.
-
- Graham C. The Information Commissioner's Office (ICO) 2012. [2020-01-20]. Anonymization: Managing Data Protection Risk Code of Practice https://ico.org.uk/media/for-organisations/documents/1061/anonymisation-....
-
- Walonoski J, Kramer M, Nichols J, Quina A, Moesel C, Hall D, Duffett C, Dube K, Gallagher T, McLachlan S. Synthea: an approach, method, and software mechanism for generating synthetic patients and the synthetic electronic health care record. J Am Med Inform Assoc. 2017 Aug 30; doi: 10.1093/jamia/ocx079. - DOI - PMC - PubMed
-
- Anderson R. Under threat: patient confidentiality and NHS computing. Drugs Alcohol Today. 2006;6(4):13–7. doi: 10.1108/17459265200600060. - DOI
-
- Ohm P. Broken promises of privacy: responding to the surprising failure of anonymization. UCLA Law Rev. 2010;57:1701. https://ssrn.com/abstract=1450006
LinkOut - more resources
Full Text Sources
