

A Mobile Phone-Based Support Intervention to Increase Use of Postabortion Family Planning in Cambodia: Cost-Effectiveness Evaluation
- PMID: 32130166
- PMCID: PMC7064963
- DOI: 10.2196/16276
A Mobile Phone-Based Support Intervention to Increase Use of Postabortion Family Planning in Cambodia: Cost-Effectiveness Evaluation
Abstract
Background: Despite progress over the last decade, there is a continuing unmet need for contraception in Cambodia. Interventions delivered by mobile phone could help increase uptake and continuation of contraception, particularly among hard-to-reach populations, by providing interactive personalized support inexpensively wherever the person is located and whenever needed.
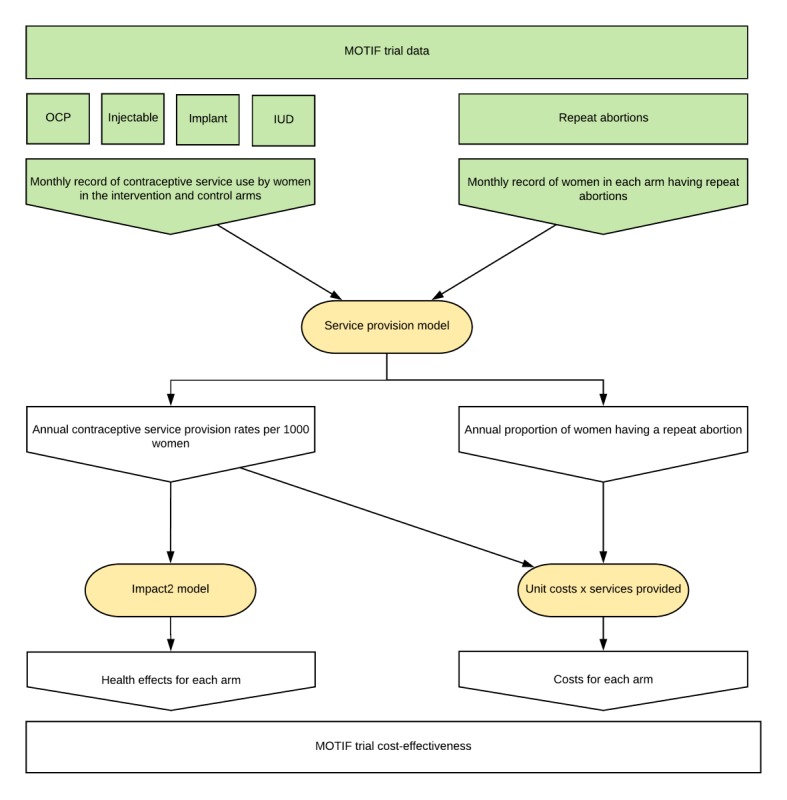
Objective: The objective of this study was to evaluate the cost-effectiveness of mobile phone-based support added to standard postabortion family planning care in Cambodia, according to the results of the MOTIF (MObile Technology for Improved Family planning) trial.
Methods: A model was created to estimate the costs and effects of the intervention versus standard care. We adopted a societal perspective when estimating costs, including direct and indirect costs for users. The incremental cost-effectiveness ratio was calculated for the base case, as well as a deterministic and probabilistic sensitivity analysis, which we compared against a range of likely cost-effectiveness thresholds.
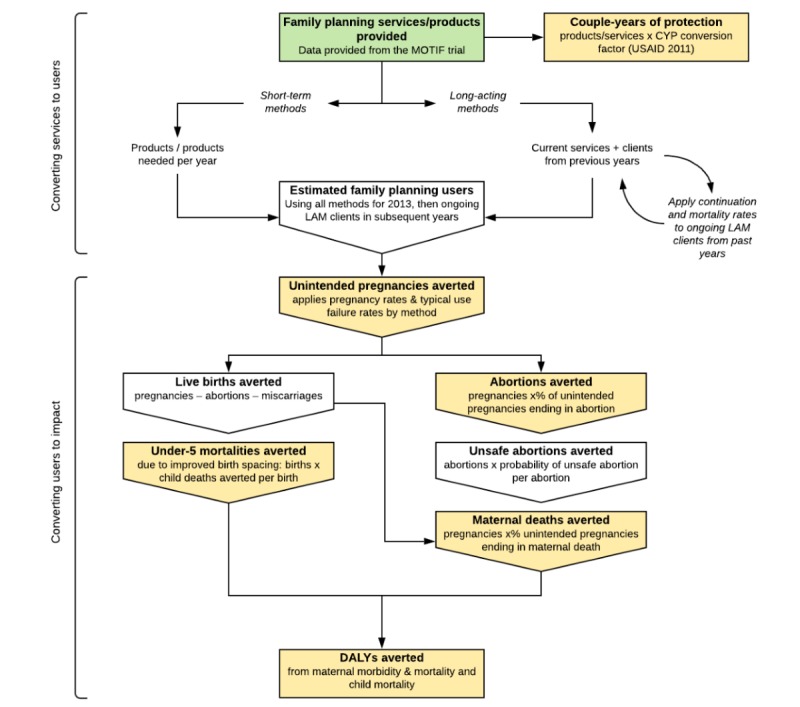
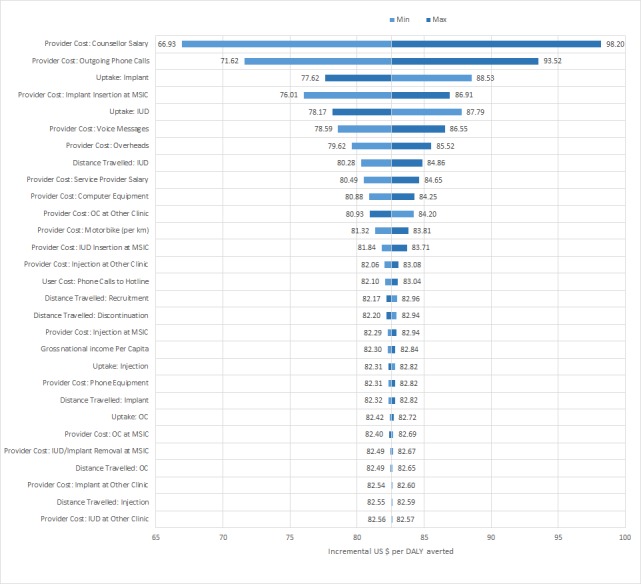
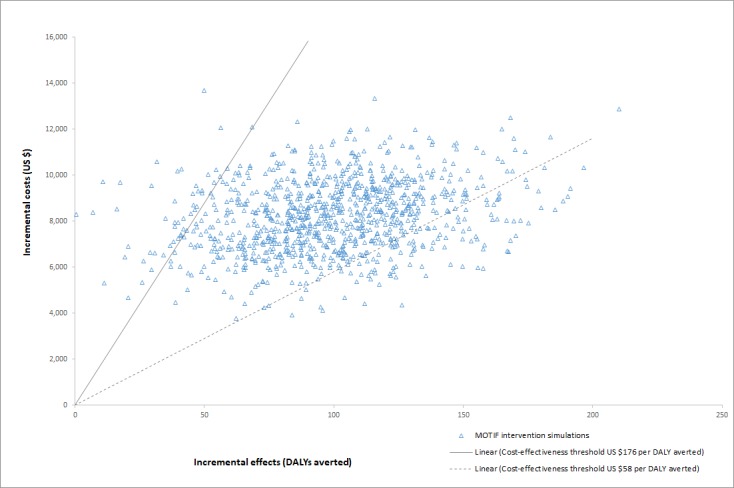
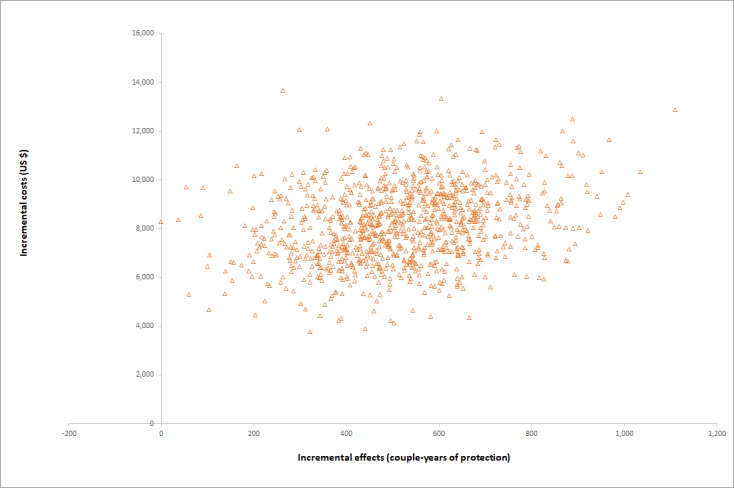
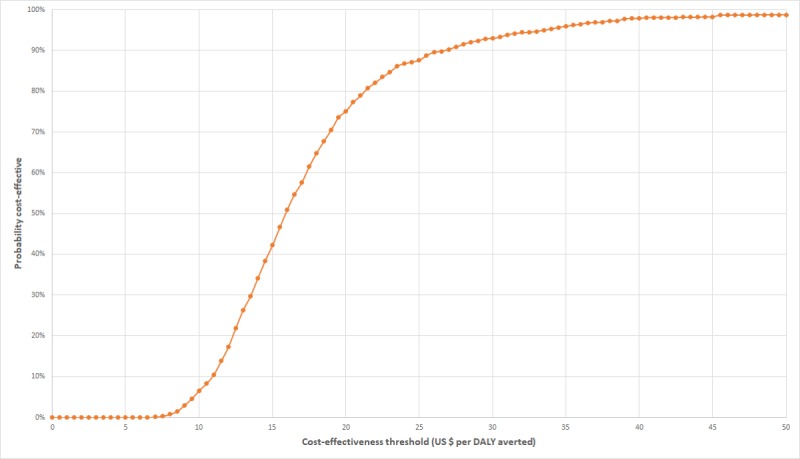
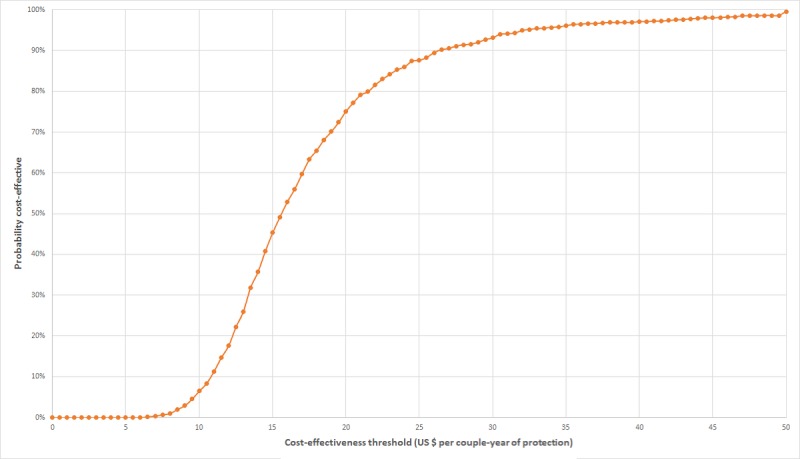
Results: The incremental cost of mobile phone-based support was estimated to be an additional US $8160.49 per 1000 clients, leading to an estimated 518 couple-years of protection (CYPs) gained per 1000 clients and 99 disability-adjusted life-years (DALYs) averted. The incremental cost-effectiveness ratio was US $15.75 per additional CYP and US $82.57 per DALY averted. The model was most sensitive to personnel and mobile service costs. Assuming a range of cost-effectiveness thresholds from US $58 to US $176 for Cambodia, the probability of the intervention being cost-effective ranged from 11% to 95%.
Conclusions: This study demonstrates that the cost-effectiveness of the intervention delivered by mobile phone assessed in the MOTIF trial lies within the estimated range of the cost-effectiveness threshold for Cambodia. When assessing value in interventions to improve the uptake and adherence of family planning services, the use of interactive mobile phone messaging and counselling for women who have had an abortion should be considered as an option by policy makers.
Trial registration: ClinicalTrials.gov NCT01823861; https://clinicaltrials.gov/ct2/show/NCT01823861.
Keywords: Cambodia; contraception; cost-effectiveness; digital health; mHealth; postabortion contraception; postabortion family planning.
©Jeremy Hill, Jourdan McGinn, John Cairns, Caroline Free, Chris Smith. Originally published in JMIR mHealth and uHealth (http://mhealth.jmir.org), 25.02.2020.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Singh S, Darroch JE, Ashford LS. Guttmacher Institute. New York: Guttmacher Institute; 2014. [2020-01-26]. Adding It Up 2014: The Costs and Benefits of Investing in Sexual and Reproductive Health https://www.guttmacher.org/report/adding-it-costs-and-benefits-investing....
-
- National Institute of Statistics/Cambodia. Directorate General for Health/Cambodia. ICF International . The DHS Program. Phnom Penh, Cambodia: National Institute of Statistics/Cambodia, Directorate General for Health/Cambodia, and ICF International; 2015. [2020-01-26]. Cambodia Demographic and Health Survey 2014 http://dhsprogram.com/publications/publication-FR312-DHS-Final-Reports.cfm.
-
- Källander K, Tibenderana JK, Akpogheneta OJ, Strachan DL, Hill Z, Asbroek AA, Conteh L, Kirkwood BR, Meek SR. Mobile health (mHealth) approaches and lessons for increased performance and retention of community health workers in low- and middle-income countries: a review. J Med Internet Res. 2013;15(1):e17. doi: 10.2196/jmir.2130. http://www.jmir.org/2013/1/e17/ - DOI - PMC - PubMed
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
