

Association of combination statin and antihypertensive therapy with reduced Alzheimer's disease and related dementia risk
- PMID: 32130251
- PMCID: PMC7055882
- DOI: 10.1371/journal.pone.0229541
Association of combination statin and antihypertensive therapy with reduced Alzheimer's disease and related dementia risk
Abstract
Background: Hyperlipidemia and hypertension are modifiable risk factors for Alzheimer's disease and related dementias (ADRD). Approximately 25% of adults over age 65 use both antihypertensives (AHTs) and statins for these conditions. While a growing body of evidence found statins and AHTs are independently associated with lower ADRD risk, no evidence exists on simultaneous use for different drug class combinations and ADRD risk. Our primary objective was to compare ADRD risk associated with concurrent use of different combinations of statins and antihypertensives.
Methods: In a retrospective cohort study (2007-2014), we analyzed 694,672 Medicare beneficiaries in the United States (2,017,786 person-years) who concurrently used both statins and AHTs. Using logistic regression adjusting for age, socioeconomic status and comorbidities, we quantified incident ADRD diagnosis associated with concurrent use of different statin molecules (atorvastatin, pravastatin, rosuvastatin, and simvastatin) and AHT drug classes (two renin-angiotensin system (RAS)-acting AHTs, angiotensin converting enzyme inhibitors (ACEIs) or angiotensin-II receptor blockers (ARBs), vs non-RAS-acting AHTs).
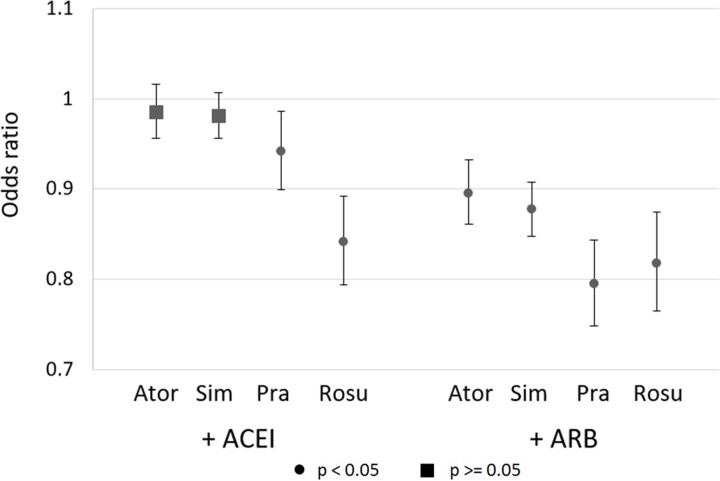
Findings: Pravastatin or rosuvastatin combined with RAS-acting AHTs reduce risk of ADRD relative to any statin combined with non-RAS-acting AHTs: ACEI+pravastatin odds ratio (OR) = 0.942 (CI: 0.899-0.986, p = 0.011), ACEI+rosuvastatin OR = 0.841 (CI: 0.794-0.892, p<0.001), ARB+pravastatin OR = 0.794 (CI: 0.748-0.843, p<0.001), ARB+rosuvastatin OR = 0.818 (CI: 0.765-0.874, p<0.001). ARBs combined with atorvastatin and simvastatin are associated with smaller reductions in risk, and ACEI with no risk reduction, compared to when combined with pravastatin or rosuvastatin. Among Hispanics, no combination of statins and RAS-acting AHTs reduces risk relative to combinations of statins and non-RAS-acting AHTs. Among blacks using ACEI+rosuvastatin, ADRD odds were 33% lower compared to blacks using other statins combined with non-RAS-acting AHTs (OR = 0.672 (CI: 0.548-0.825, p<0.001)).
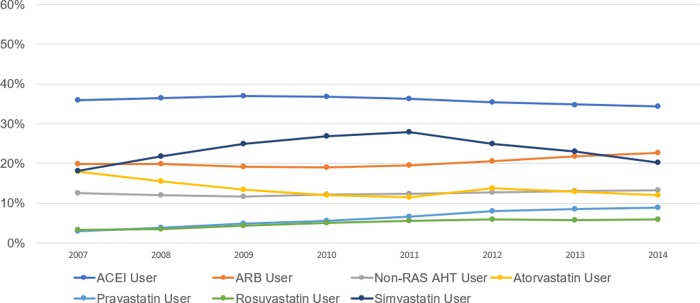
Conclusion: Among older Americans, use of pravastatin and rosuvastatin to treat hyperlipidemia is less common than use of simvastatin and atorvastatin, however, in combination with RAS-acting AHTs, particularly ARBs, they may be more effective at reducing risk of ADRD. The number of Americans with ADRD may be reduced with drug treatments for vascular health that also confer effects on ADRD.
Conflict of interest statement
Partial financial support for this research was provided by Amgen. This does not alter our adherence to PLOS ONE policies on sharing data and materials. The company had no role in any stage of the research process. The concept, design, acquisition, analysis, and interpretation of data, manuscript drafting, and revisions, were completed without any involvement from the company.
Figures
References
-
- Livingston G., et al. Dementia prevention, intervention, and care. The Lancet, 2017. 390(10113): p. 2673–2734. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
