

Drooling in Parkinson's Disease: Prevalence and Progression from the Non-motor International Longitudinal Study
- PMID: 32130515
- PMCID: PMC7669801
- DOI: 10.1007/s00455-020-10102-5
Drooling in Parkinson's Disease: Prevalence and Progression from the Non-motor International Longitudinal Study
Abstract
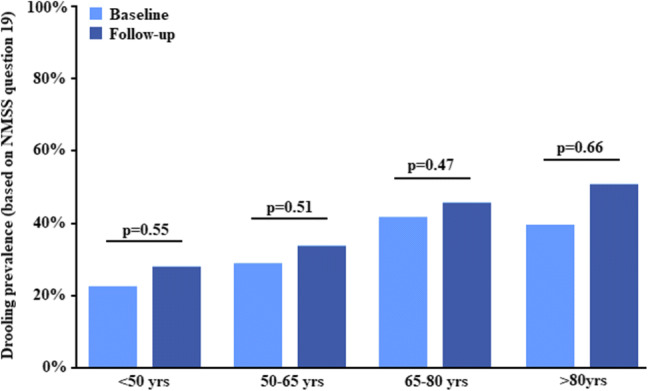
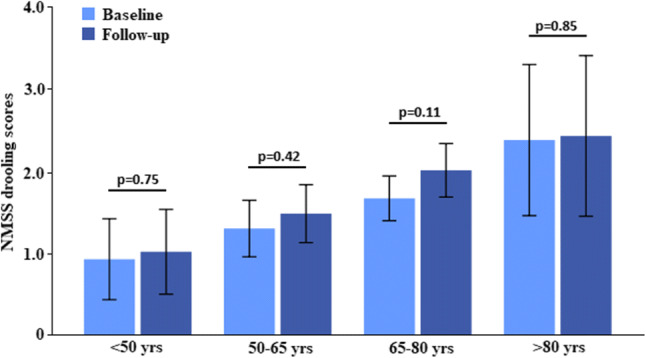
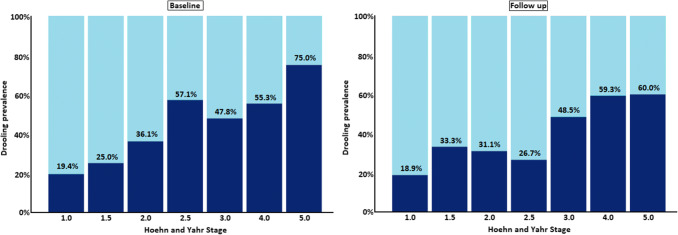
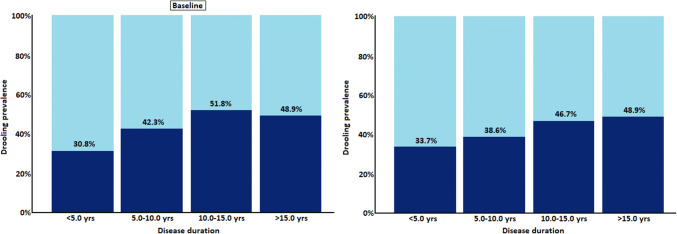
Sialorrhoea in Parkinson's disease (PD) is an often neglected yet key non-motor symptom with impact on patient quality of life. However, previous studies have shown a broad range of prevalence figures. To assess prevalence of drooling in PD and its relationship to quality of life, we performed a retrospective analysis of 728 consecutive PD patients who had a baseline and follow-up assessment as part of the Non-motor International Longitudinal Study (NILS), and for whom drooling presence and severity were available, assessed through the Non-Motor Symptoms Scale (NMSS). In addition, we analysed the prevalence of associated dysphagia through self-reported outcomes. Quality of life was assessed through the PDQ-8 scale. Baseline (disease duration 5.6 years) prevalence of drooling was 37.2% (score ≥ 1 NMSS question 19), and after 3.27 ± 1.74 years follow-up, this was 40.1% (p = 0.17). The prevalence of drooling increased with age (p < 0.001). The severity of drooling, however, did not change (p = 0.12). While in 456 patients without drooling at baseline, only 16% (n = 73) had dysphagia (question 20 of the NMSS), in those with drooling this was 34.3% (p < 0.001). At follow-up, the number of patients with dysphagia had increased, 20.4% with no drooling had dysphagia, and 43.6% with drooling had dysphagia. Both at baseline and follow-up, drooling severity was significantly positively associated with quality of life (PDQ-8; r = 0.199; p < 0.001). In moderately advanced PD patients, subjective drooling occurs in over one-third of patients and was significantly associated with decreased quality of life. Dysphagia occurred significantly more often in patients with drooling.
Keywords: Deglutition; Deglutition disorders; Drooling; Dysphagia; Non-motor symptoms scale; Parkinson’s disease.
Conflict of interest statement
The authors declare that there are no conflicts of interest relevant to this work. Financial disclosures not related to this work: Dr. van Wamelen reports grants and personal fees from Britannia Pharmaceuticals, personal fees from Invisio Pharmaceuticals, outside the submitted work. Dr. Leta reports personal fees from Britannia Pharmaceuticals, personal fees from Invisio Pharmaceuticals, grants from Parkinson's UK, grants from Bial, outside the submitted work. Mrs. Johnson has nothing to disclose. Dr. Lazcano-Ocampo has nothing to disclose. Ms. Podlewska reports personal fees from Britannia Pharmaceuticals, grants from Welcome Trust, outside the submitted work. Dr. Rukavina has nothing to disclose. Mrs. Rizos has nothing to disclose. Prof. Martinez-Martin reports personal fees from Editorial Viguera, grants and personal fees from International Parkinson and Movement Disorder Society, personal fees from HM Hospitales de Madrid, other from King's Parkinson's Disease Pain scale, outside the submitted work. Prof. Ray Chaudhuri reports personal fees from Abbvie, personal fees from Britannia Pharmaceuticals, personal fees from UCB, personal fees from Mundipharma, personal fees from Zambon, personal fees from Global Kinetics, personal fees from Bial, grants from Parkinson's UK, grants from NIHR, grants from PDNMG, grants from Kirby Laing, grants from NPF, other from AbbVie, other from UCB, other from Sunovion, other from Pfizer, other from Jazz Pharma, from Bial, from Global Kinetics, grants from Welcome Trust, outside the submitted work.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
