

Exosomes: From Potential Culprits to New Therapeutic Promise in the Setting of Cardiac Fibrosis
- PMID: 32131460
- PMCID: PMC7140485
- DOI: 10.3390/cells9030592
Exosomes: From Potential Culprits to New Therapeutic Promise in the Setting of Cardiac Fibrosis
Abstract
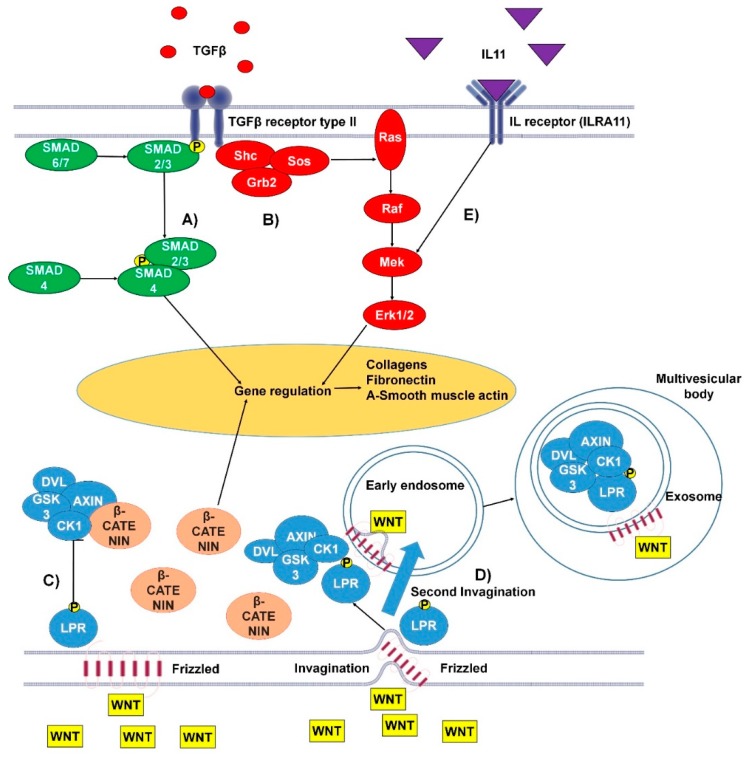
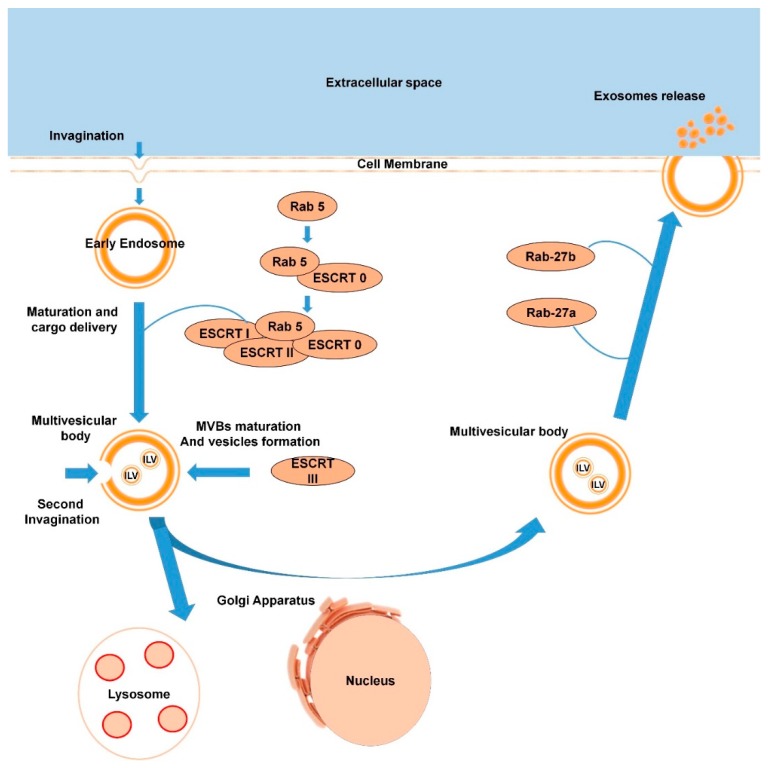
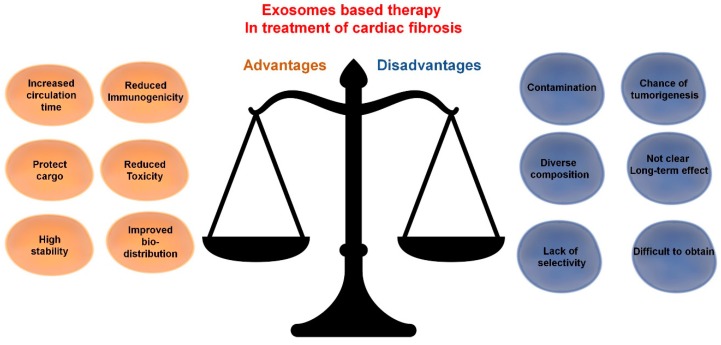
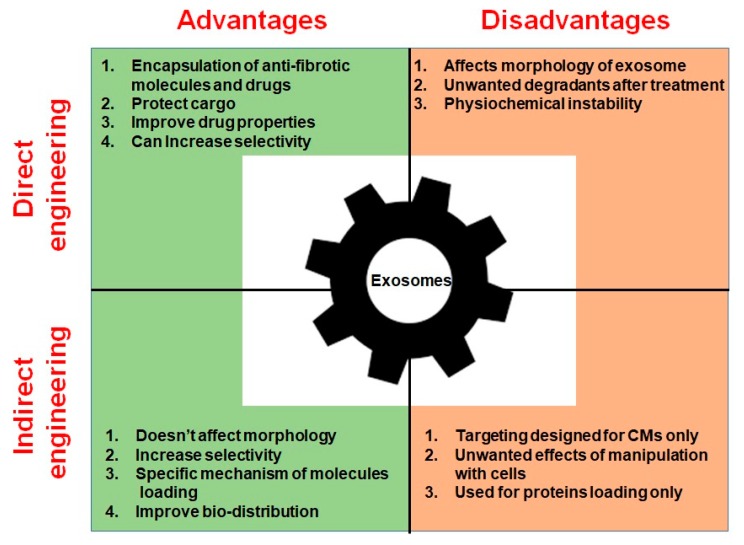
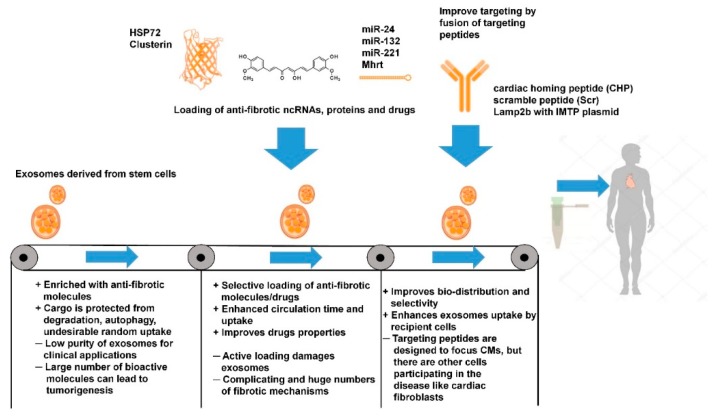
Fibrosis is a significant global health problem associated with many inflammatory and degenerative diseases affecting multiple organs, individually or simultaneously. Fibrosis develops when extracellular matrix (ECM) remodeling becomes excessive or uncontrolled and is associated with nearly all forms of heart disease. Cardiac fibroblasts and myofibroblasts are the main effectors of ECM deposition and scar formation. The heart is a complex multicellular organ, where the various resident cell types communicate between themselves and with cells of the blood and immune systems. Exosomes, which are small extracellular vesicles, (EVs), contribute to cell-to-cell communication and their pathophysiological relevance and therapeutic potential is emerging. Here, we will critically review the role of endogenous exosomes as possible fibrosis mediators and discuss the possibility of using stem cell-derived and/or engineered exosomes as anti-fibrotic agents.
Keywords: EVs engineering; cardiac fibrosis; exosomes; extracellular vesicle (EVs); heart failure; microRNAs; noncoding RNAs; stem cells.
Conflict of interest statement
The authors declare that there is no conflict of interest regarding the publication of this article.
Figures
References
-
- Gulati A., Japp A.G., Raza S., Halliday B.P., Jones D.A., Newsome S., Ismail N.A., Morarji K., Khwaja J., Spath N., et al. Absence of Myocardial Fibrosis Predicts Favorable Long-Term Survival in NewOnset Heart Failure. Circulation. 2018;11:e007722. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
