

Sarcopenia as a predictor of mortality in women with breast cancer: a meta-analysis and systematic review
- PMID: 32131764
- PMCID: PMC7057618
- DOI: 10.1186/s12885-020-6645-6
Sarcopenia as a predictor of mortality in women with breast cancer: a meta-analysis and systematic review
Abstract
Background: Breast cancer is the most commonly diagnosed cancer and the leading cause of cancer death in women worldwide. Recently, studies have been published with inconsistent findings regarding whether sarcopenia is a risk factor for mortality in breast cancer patients. Therefore, the aim of this systematic review and meta-analysis was to systematically assess and quantify sarcopenia as a risk factor for mortality in breast cancer patients.
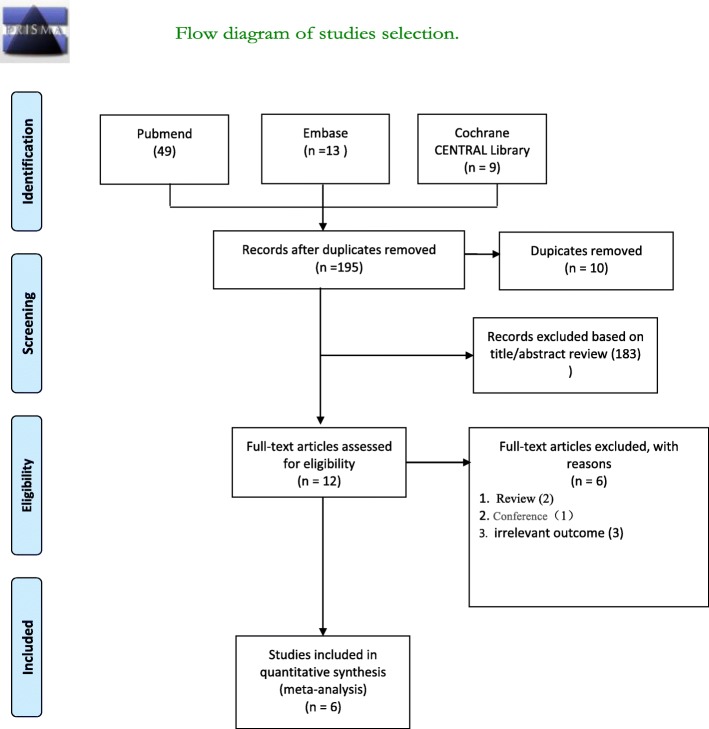
Methods: In a systematic literature review of PubMed, EMBASE, and the Cochrane CENTRAL Library, we searched for observational studies written in English (from database inception until April 30, 2019) that reported an association between sarcopenia and breast cancer in women who were 18 years or older.
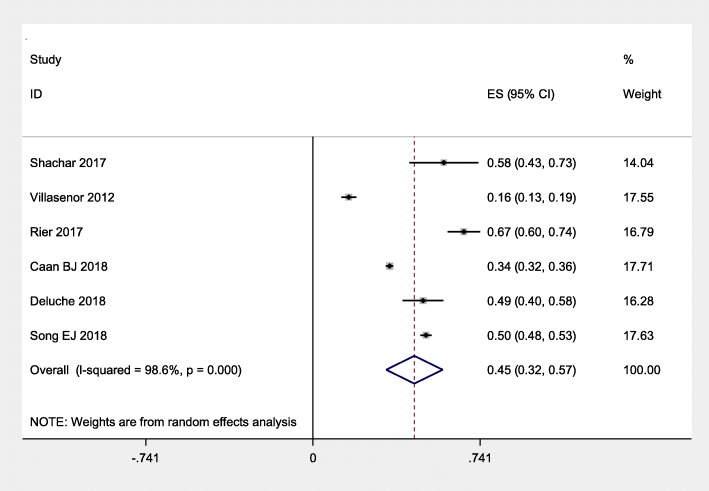
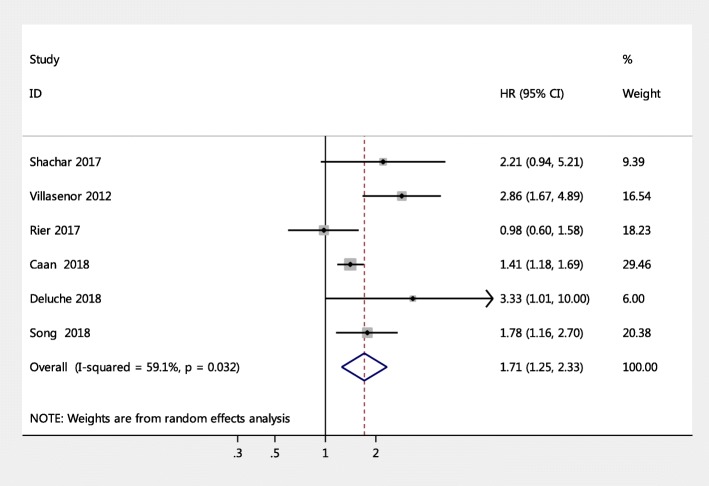
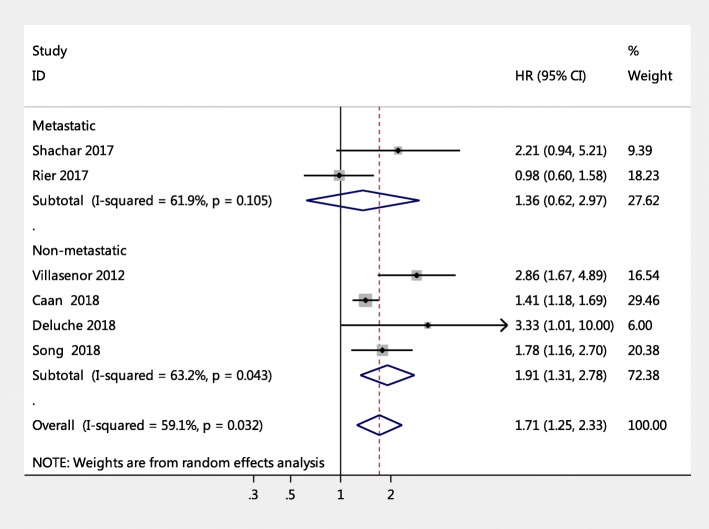
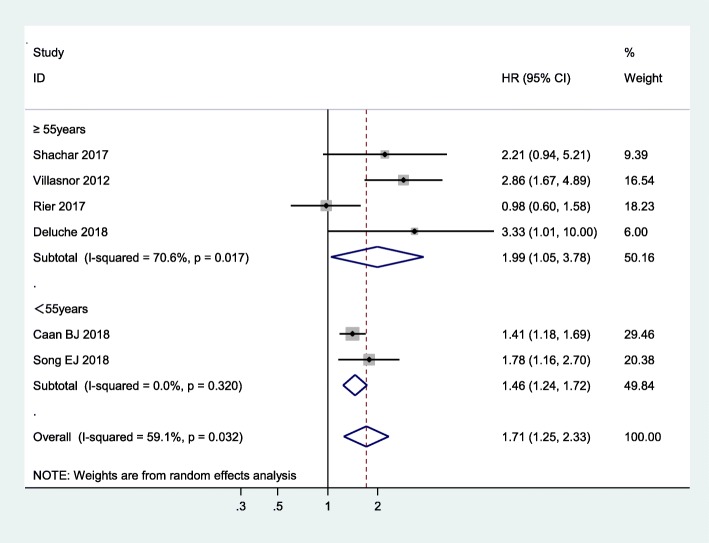
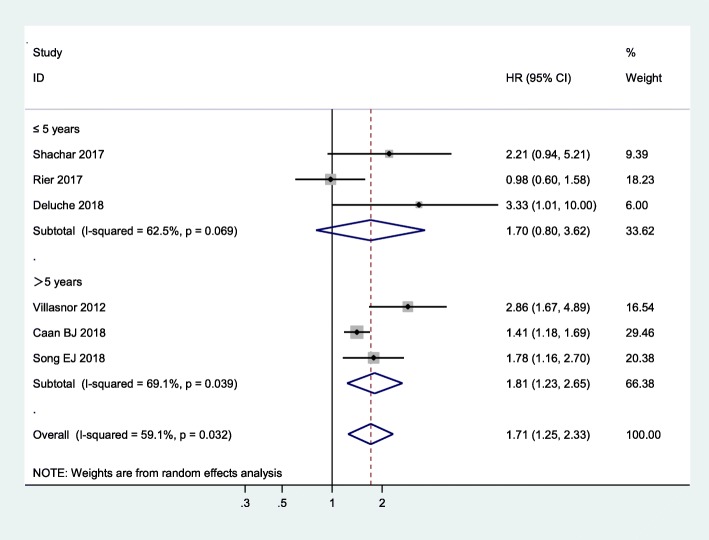
Results: A total of six studies (5497 participants) were included in this meta-analysis. Breast cancer patients with sarcopenia were associated with a significantly higher risk of mortality, compared to breast cancer patients without sarcopenia (pooled HR-hazard ratio = 1.71, 95% CI: 1.25-2.33, I2 = 59.1%). In addition, the results of age subgroup analysis showed that participants younger than 55 years with sarcopenia had a lower risk of mortality than participants aged 55 years and older with sarcopenia (pooled HR = 1.46, 95% CI: 1.24-1.72 versus pooled HR = 1.99, 95% CI: 1.05-3.78), whereas both have an increased risk of mortality compared to non-sarcopenic patients. Subgroup analyses regarding stage at diagnosis revealed an increased risk of mortality in non-metastatic patients compared to participants without sarcopenia (pooled HR = 1.91, 95% CI: 1.32-2.78), whereas the association was not significant in metastatic breast cancer patients. Other subgroup analyses were performed using different follow-up periods (> 5 years versus ≤5 years) and the results were different (pooled HR = 1.81, 95% CI: 1.23-2.65 versus pooled HR = 1.70, 95% CI: 0.80-3.62).
Conclusions: The present study found that sarcopenia is a risk factor for mortality among female early breast cancer patients. It is imperative that more research into specific interventions aimed at treating sarcopenia be conducted in the near future in order to provide evidence which could lead to decreased mortality rates in breast cancer patients.
Keywords: Breast cancer; Mortality rate; Sarcopenia; Systematic review and meta-analysis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
