

Improving the healthcare response to domestic violence and abuse in UK primary care: interrupted time series evaluation of a system-level training and support programme
- PMID: 32131828
- PMCID: PMC7057596
- DOI: 10.1186/s12916-020-1506-3
Improving the healthcare response to domestic violence and abuse in UK primary care: interrupted time series evaluation of a system-level training and support programme
Abstract
Background: It is unknown whether interventions known to improve the healthcare response to domestic violence and abuse (DVA)-a global health concern-are effective outside of a trial.
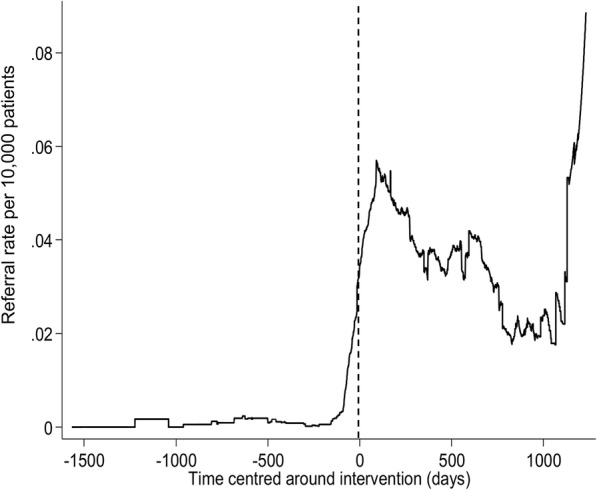
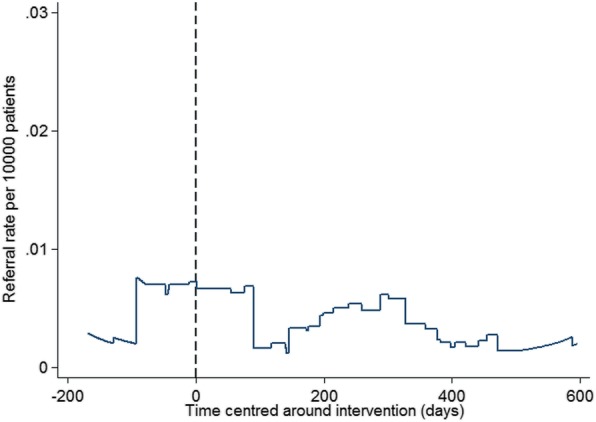
Methods: An observational interrupted time series study in general practice. All registered women aged 16 and above were eligible for inclusion. In four implementation boroughs' general practices, there was face-to-face, practice-based, clinically relevant DVA training, a prompt in the electronic medical record, reminding clinicians to consider DVA, a simple referral pathway to a named advocate, ensuring direct access for women to specialist services, overseen by a national, health-focused DVA organisation, fostering best practice. The fifth comparator borough had only a session delivered by a local DVA specialist agency at community venues conveying information to clinicians. The primary outcome was the daily number of referrals received by DVA workers per 1000 women registered in a general practice, from 205 general practices, in all five northeast London boroughs. The secondary outcome was recorded new DVA cases in the electronic medical record in two boroughs. Data was analysed using an interrupted time series with a mixed effects Poisson regression model.
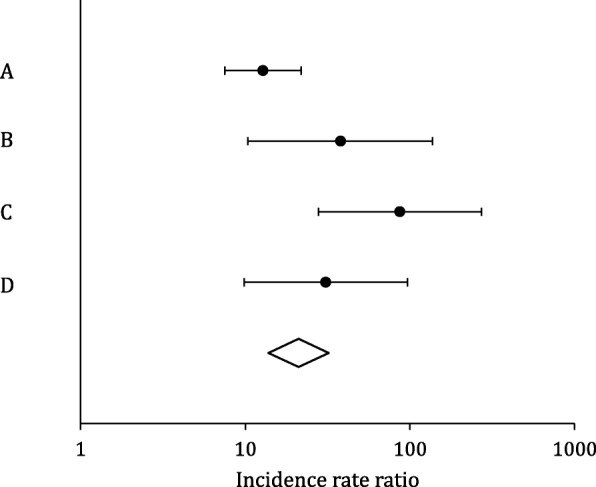
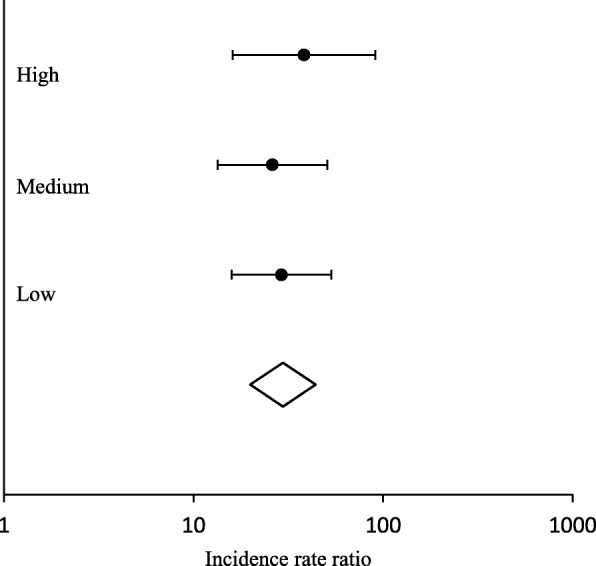
Results: In the 144 general practices in the four implementation boroughs, there was a significant increase in referrals received by DVA workers-global incidence rate ratio of 30.24 (95% CI 20.55 to 44.77, p < 0.001). There was no increase in the 61 general practices in the other comparator borough (incidence rate ratio of 0.95, 95% CI 0.13 to 6.84, p = 0.959). New DVA cases recorded significantly increased with an incident rate ratio of 1.27 (95% CI 1.09 to 1.48, p < 0.002) in the implementation borough but not in the comparator borough (incidence rate ratio of 1.05, 95% CI 0.82 to 1.34, p = 0.699).
Conclusions: Implementing integrated referral routes, training and system-level support, guided by a national health-focused DVA organisation, outside of a trial setting, was effective and sustainable at scale, over four years (2012 to 2017) increasing referrals to DVA workers and new DVA cases recorded in electronic medical records.
Keywords: Complex; Domestic violence abuse; Evaluation; Implementation; Improvement; Interrupted time-series; Observational.
Conflict of interest statement
AH and MJ were DVA IRIS advocate educators, at the time of original IRIS trial, and are now both funded to facilitate IRIS dissemination in the UK, with MJ the CEO of IRISi, a national, health-focused DVA social enterprise. Positive trial findings would support their career development. GF is a non-executive IRISi board member. All other authors declare that they have no competing interests.
Figures
References
-
- WHO . Responding to intimate partner violence and sexual violence against women: WHO clinical and policy guidelines. 2013. - PubMed
-
- National Institute for Health and Care Excellence . Domestic violence and abuse: multi- agency working NICE guideline. 2014.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
